


Research Article - (2024) Volume 2, Issue 1
Analysis of Renal Function in COVID-19 Positive Tunisians Patients
2Faculty of Pharmacy, Department of Biology, University of Monastir, Tunisia
3Faculty of Medicine, LR99ES09 Laboratory of Antibiotic Resistance, University of Tunis El Manar, Tun, Tunisia
4Higher Institute of Biotechnology Sidi Thabet Manouba University, Ariana, Tunisia
Received Date: Jan 10, 2024 / Accepted Date: Feb 10, 2024 / Published Date: Mar 04, 2024
Copyright: ©Â©2024 Hajer Kilani, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nakaa, H., Kilani, H., Kaoual, S., Chatti, L., Jemaa, R. B., et al. (2024). Analysis of Renal Function in COVID-19 Positive Tunisians Patients. Trans Med OA, 2(1), 1-6.
Abstract
Background: The objective of this study was to evaluate an analysis of renal function in covid-19 positive patients among their hospitalization period.
Methods: Biochemical analyzes of three analyzes (Urea, Creatinine and Blood Ionogram) of the 10 COVID-19 positive patients hospitalized at Orthopedic Institute of Med Kassab during the month of April. 4 out of 10 people had acute kidney failure during this period of hospitalization.
Results: The four out of ten COVID-19 positive people had signs of kidney damage reflected by fluctuations in the values of biological parameters.
Conclusion: Monitoring the evolution of urea, creatinine and blood ionogram values alone is not sufficient and it is necessary to detect other more valuable parameters.
Keywords
Diagnostics, Sars-Cov-2, Tunisia , Biochemical analyzes, Blood.
Introduction
The COVID-19 pandemic first emerged in December 2019 in China, and then rapidly spread to other countries in the world including Tunisia [1]. Several studies have shown extremely common kidney damage in patients with COVID-19. It can present in the form of acute renal failure (5-35% of patients), hematuria (30-40%) and/or proteinuria (40-65%). PCR analysis of organs from patients who died from COVID-19 revealed that the kidneys are among the target organs most frequently affected by the virus, after the lungs. The high frequency of kidney damage is explained by the presence of the viral ACE2 receptor (angiotensinconverting enzyme 2) and its co-receptors on the surface of the kidney (figure 1). Diagram of a nephron, with glomerulus, and the respective cells (podocyte and tubular cell) potentially targets of SARS-CoV-2; B: Attachment of the virus to the ACE2 receptor (expressed on tubular cells and podocytes), via the S protein (“spike”) carried by the protuberances; C: The S Protein – ACE2 receptor couple is internalized by an endosome vesicle [2]. The RNA is released [3]. It is a pathological condition during which the kidneys are unable to ensure blood filtration. This is expressed by an imbalance of water and minerals in the body, which can lead to a fatal situation. The measurement of Urea and Creatinine in the blood of patients helps to evaluate renal function, particularly the presence of renal insufficiency [4]. It allows us to estimate the proper functioning of the kidney which is used to eliminate nitrogenous waste and many other substances. It also helps control the acid-base balance to maintain a neutral pH, without forgetting the metabolism of electrolytes [5].
Figure 1: A: Diagram of a nephron, with glomerulus, and the respective cells (podocyte and tubular cell) potentially targets of SARS-CoV-2; B: Attachment of the virus to the ACE2 receptor (expressed on tubular cells and podocytes), via the S protein (“spike”) carried by the protuberances; C: The S Protein – ACE2 receptor couple is internalized by an endosome vesicle. The RNA is released.
Urea is a molecule that results from a process of protein degradation. It is the main form of elimination of nitrogenous waste, through urine. Creatinine is a waste product of the body which comes from the breakdown of creatine which plays a role in muscle contraction. It is eliminated in the urine by filtration through the kidneys. When the kidneys' ability to eliminate waste decreases, the amount of creatinine increases in the blood. Blood ionogram is an essential examination to monitor the general functioning of our body and which makes it possible to reveal numerous pathologies which could go unnoticed, in particular any kidney dysfunction [5]. Kalemia: this is the dosage of potassium (K+) in the blood. It plays a role in maintaining the difference in concentrations between the intra and extra cellular environment, it is at the origin of an action potential and subsequently the activation of nerve and muscle cells. Its normal value between 3.5-5 mEq.L-1 [5]. Natremia: it is the dosage of sodium (Na+) in the blood: this molecule participates in the control and balance of the volume of the extra-cellular environment, in the maintenance of the electrochemical gradient of the cells, in the transmission of nerve impulses , muscle contraction and intestinal absorption of certain nutrients. Its normal value between 136-145 mEq.L-1 [3]. Chloremia: it is the dosage of Chlorine (Cl-) in the blood. It is found in the extracellular liquids associated with sodium and potassium, it allows the hydration of the body and to control osmotic pressure and regulation pH. Its normal value between 98-108 mEq.L-1 [5].
Materials and Methods
Pre-Analytical Phase
Blood Sampling
A simple sample of 4 ml of blood from a venous blood vessel in a tube with Lithium Heparin from 10 patients hospitalized at IMKO.
Centrifugation
The blood serum is separated from the pellet by a centrifuge by accelerating the sedimentation of the heavy components for 10 minutes.
Analytical Phase
A ROCHE COBAS INTEGRA 400 PLUS chemistry analyzer, which undergoes continuous calibration and monitoring (normal and pathological) is used to determine the concentrations of urea and creatinine present in the plasma of our samples and provides us with information on their values. accurate and valuable samples. The EASYLYTE Na +/ k+ /Cl- is a calibrated and controlled analyzer used to quantitatively determine the concentration of Na+, K+ and Cl- ions in the plasma of samples using a selective membrane of specific electrodes
Results and discussion:
This study is established by biochemical analyzes of three analyzes (Urea, Creatinine and Blood Ionogram) of the 10 COVID-19 positive patients hospitalized at Orthopedic Institute of Med Kassab during the month of April. 4 out of 10 people had acute kidney failure during this period of hospitalization. We take the following usual values: creatinine (7-11 mg/L); urea (≤0.498g/L); Na+ (136-145 mEq.L-1); K+ (3.5-5mEq.L-1); Cl- (98-108mEq.L-1). Patient 1, aged 85 has kidney damage from day 1 of hospitalization with a creatinine estimated at 20.22 mg/L. this value then decreased without normalizing [7 - 11 mg/L], then it increased again to reach 22.37 mg/L on day 8. Urea also increased in parallel with creatinine to reach a value of 1.69 g/L on day 9 of hospitalization. The blood ionogram showed a fluctuation in the values of serum sodium, chloremia due to a hydration disorder in the patient, sepsis and probably from acute kidney injury (figure 2, figure 3). Patient 2, aged 58, was initially, creatinine and urea were normal. On day 9 of hospitalization, these 2 parameters increased successively to reach 54.9 mg/L and 1.8g/L then they gradually decreased. At the same time, serum potassium increased following an alteration of renal cells and serum sodium and chloremia remained normal (figure 2, figure 3).
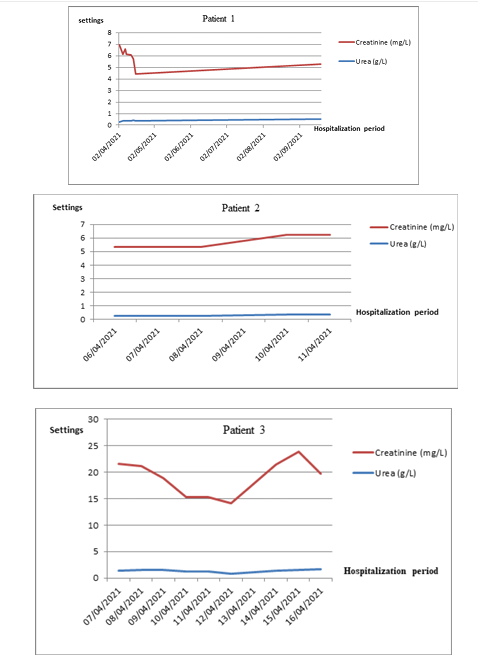
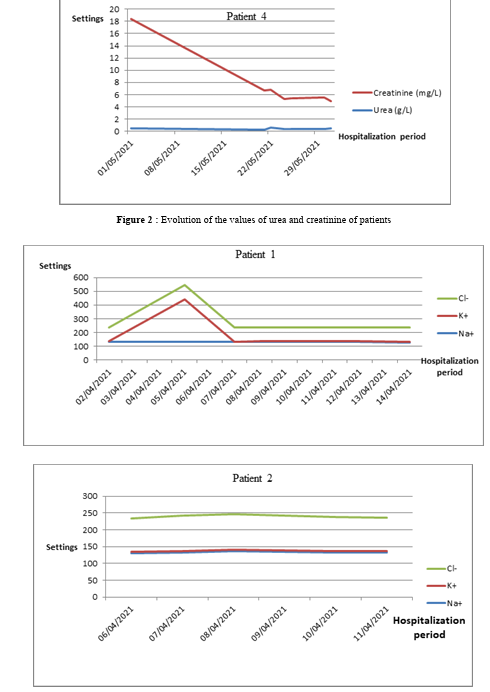
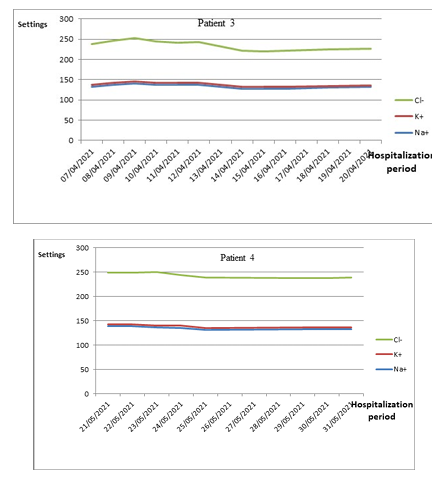
Figure 3 : Evolution of the values of blood ionogram (Na+, K+ and Cl-) of patients
Patient 3, aged 60, in the first days of hospitalization, creatinine and urea values were very high compared to usual values. Creatinine reached a maximum equal to 14.012 mg/L and urea reached a maximum equal to 0.593g/L. the patient had hypercreatininemia and hyperuremia. The ionogram shows hyponatremia followed by hypochloremia due to poor renal filtration resulting in overhydration. but normal serum potassium (figure 2, figure 3). Patient 4 aged 70 suffered hypercreatininemia with a maximum value estimated at 10.622 mg/L on the last day, followed by hyperuremia with a maximum value equal to 0.913 g/L on the first two days. The blood ionogram shows hyponatremia with values varying between 128 and 135 mEq.L-1 and hypochloremia due to overhydration caused by an alteration in renal filtration function. The serum potassium remained normal (figure 2, figure 3) [5]. The four out of ten COVID-19 positive people had signs of kidney damage reflected by fluctuations in the values of biological parameters. Hence the confirmation that the kidneys are the target organs of contagion after the lungs. And that it causes harmful effects on kidney cells and their absorption or filtration function. Monitoring the evolution of urea, creatinine and blood ionogram values alone is not sufficient and it is necessary to detect other more valuable parameters such as hematuria, proteinuria, clearance, diuresis and Urine ionogram with an increase in the number of patients [5].
Conclusion
It is necessary to know how to assess the old or recent nature of the disturbance in the biological parameters studied and check the morphological state of the kidneys by ultrasound to distinguish between acute or chronic renal failure, taking into account that these patients had an average age ≥50 years.
Authors Contributions
Study concept and drafting of the manuscript were done by Kilani Hajer, Hadhemi Nakaa, Lamia Chatti, Salma Kaoual, Rim Ben Jemaa Driouich Chaouachi and Sophia Bouhalila Besbes Acquisition, analysis, and interpretation of data were performed by Hadhemi Nakaa, Kilani Hajer Critical revision of the manuscript for important intellectual content was conducted by Sophia Bouhalila Besbes.
Conflict of interest
None of the authors of this paper has a financial or personal relationship with other people or organizations that could in appropriately influence or bias the content of the paper.
Funding
This work was supported by the Tunisian ministry of Health
Acknowledgements
The laboratory is financed by the Ministry of Health according to a national strategy of diagnostic COVID 19.
References
- Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J.,... & Tan, W. (2020). A novel coronavirus from patients with pneumonia in China, 2019. New England journal of medicine, 382(8), 727-733.
- Rahimi, A., Mirzazadeh, A., & Tavakolpour, S. (2021). Genetics and genomics of SARS-CoV-2: A review of the literature with the special focus on genetic diversity and SARS-CoV-2 genome detection. Genomics, 113(1), 1221-1232.
- Amir, I. J., Lebar, Z., & Mahmoud, M. (2020). Covid-19: virologie, épidémiologie et diagnostic biologique. Option/ Bio, 31(619), 15.
- Ketfi, A., Chabati, O., Chemali, S., Mahjoub, M., Gharnaout, M., Touahri, R., ... & Saad, H. B. (2020). Profil clinique, biologique et radiologique des patients Algériens hospitalisés pour COVID-19: données préliminaires. The Pan African Medical Journal, 35(Suppl 2).
- Berthélémy, S. (2015). Le bilan rénal. Actualités Pharmaceutiques, 54(549), 55-58.