
COVID Research: Open Access(CROA)
ISSN: 2995-7826 | DOI: 10.33140/CROA


Research Article - (2024) Volume 2, Issue 3
An Assessment of the Effect of Coronavirus Disease 2019 (Covid-19) on Community Pharmacy Service Delivery in Lagos State
Received Date: Oct 07, 2024 / Accepted Date: Nov 04, 2024 / Published Date: Nov 27, 2024
Copyright: ©©2024 Olufunke G. Ajibola, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Ajibola, O. G., Joda, A. (2024). An Assessment of the Effect of Coronavirus Disease 2019 (Covid-19) on Community Pharmacy Service Delivery in Lagos State. COVID Res OA, 2(3), 01-13.
Abstract
Background Community pharmacists play an important role as frontline health care workers during the COVID-19 pandemic. Therefore, the delivery of pharmaceutical care and the availability of drugs is compromised. The objective of this study was to evaluate the effect of coronavirus disease 2019 (COVID-19) on community pharmacy service delivery in Lagos state.
Methods A cross-sectional study with an online questionnaire created using Google Forms software was sent to community pharmacists in Lagos State, Nigeria via the Association of Community Pharmacists in Nigeria WhatsApp platforms. The sample size was 120 respondents conveniently chosen. Ethical approval was obtained from Health Research Ethics Committee, Lagos University Teaching Hospital (LUTH), Idi-Araba, Lagos State. Collected data was analyzed using Microsoft Excel.
Results A total of 125 respondents participated in the study. The result showed 56% were female respondents and the mean age of respondents was 32.4 ± 4.7 years. Measures such as the use of face masks (90.4%) and restricted number of patients for access at a time (89.6%) were implemented to reduce the spread of COVID-19. Majority of the respondents (61.6%) believe the measures have reduced the interaction between patients and pharmacists. Most of the respondents (81.6%) believe the pandemic has affected the availability and almost average (48%) of the respondents think that there was inflation in the prices of products like antimalarials, antibiotics, protective and preventive equipment and multivitamins.
Conclusion The COVID-19 pandemic has affected the delivery of pharmaceutical care to clients as well as the availability of medicines to patients. To improve the delivery of pharmaceutical care, tele-pharmacy and online pharmaceutical services may be employed.
Keywords
Community Pharmacists, Coronavirus Disease, Pharmaceutical CareIntroduction
The coronavirus disease 2019 (COVID-19) is a global health pandemic that has resulted in a surge in the demand for frontline healthcare personnel to meet patient care needs. It is a newly identified coronavirus that causes infectious sickness [1]. The virus primarily affects the respiratory system. Fever, dry cough, muscle soreness, exhaustion, anorexia and shortness of breath are the most common symptoms [2]. Droplets from the nose or mouth are the primary mechanism of transfer from person to person. According to studies, even asymptomatic patients can spread the infection [3].
In Nigeria, about 206,279 cases of COVID-19 have been confirmed, with 194,167 patients discharged and 2,723 deaths confirmed as at October 4, 2021 [4]. Vaccines and therapies are being developed by some scientists and the biomedical research community. Currently, short-term remedies for those that require it have centered on the use of existing antivirals (like remdesivir) that have been licensed for other illnesses off-label. Some drugs are now being tested in clinical trials to determine their efficacy and safety in the treatment of COVID-19 [5]. Examples of these drugs include antiviral agents like molnupiravir and favipiravir, nitazoxanide, niclosamide, immunomodulators (infliximab, abatacept and cenicriviroc) and corticosteroids.
According to WHO (1994), community pharmacists are the most accessible health care professionals to the general populace. Community pharmacists assist patients by filling prescriptions, dispensing medications, educating and assessing patients for chronic drug renewal, providing minor illness consultations, patient monitoring and examination [6]. Community pharmacists are often the first point of contact with the health system for those with COVID-19-related health concerns or those who seek credible information and advice during this pandemic [7]. Community pharmacists are facing a lot of issues as a result of the pandemic in terms of ensuring patient care. These include assistance with infection prevention, supply chain management, stockpile prevention, and the dissemination of evidence-based medical information [8]. Both pharmacists and patients are affected by these issues.
A previous study by [9]. was concerned with the role of community pharmacies on the frontline of health service delivery against COVID-19. They ignore the important factor of how the pandemic has affected (and is still affecting) the delivery of services by the community pharmacist to patients. COVID-19 pandemic is placing extraordinary and sustained demands on the health system and providers of essential community services [10]. The pharmacist at the frontline plays a role in providing medications and counseling to the patients, therefore community pharmacies remained open during the early active phase of pandemic and continue to stay open to attend to patients and clients.
The rapid evolution of the COVID-19 pandemic has brought about a series of changes in the community pharmacy sector. In relation to the pandemic, the Center for Disease Control (CDC) published guidelines that highlight key activities of the pharmacist in helping to curb the spread of COVID-19 [11]. These guidelines have caused changes to the delivery of services to patients in the pharmacy. One of such guidelines is the practice of social distancing. Pharmacists adapted their premises to achieve this measure by ensuring the use of face masks, installing barriers and floor markers to instruct waiting patients to remain six feet away from the counter or from other patients or staff. Pharmacists also restricted patient numbers for access and implemented delivery services to patients at home, especially elderly patients who have been advised to stay at home.
Therefore, this study is aimed at assessing the effects of COVID-19 on the delivery of pharmaceutical services by community pharmacists and how pharmacists have adapted to the situation in order to satisfy customers and also curb the spread of COVID-19. The main focus includes the delivery of pharmaceutical care to patients, the availability of drugs and the price of drugs amidst the COVID-19 pandemic.
Pharmaceutical care is based on the responsible provision of drug therapy for the purpose of achieving definite outcomes which improve patient’s quality of life. Little or no study has taken into account the effects of the COVID-19 pandemic on community pharmacy services in the aspects of provision of pharmaceutical care and drug availability and prices, as these factors are crucial to both patients and pharmacists. Therefore, this study will be a useful baseline study for other researchers in this field.
The main objective of this study is to evaluate the effects of the coronavirus 2019 pandemic on community pharmacy activities.
The specific objectives are to:
1. Evaluate the changes caused by COVID-19 on community pharmacies with respect to delivery of pharmaceutical care and availability of medications to patients.
2. Assess how these changes (if any) have affected the delivery of pharmaceutical care to patients.
3. Assess how these changes have affected the availability and price of drugs in the pharmacy.
4. Evaluate how pharmacists have adapted to these changes in order to ensure adequate provision of patient care.
This research focuses on community pharmacies in Lagos state. In light of the ongoing pandemic, the study will employ an electronic format to reach the target population.
Materials and Methods
Study Setting
The study was carried out in Lagos state, located in the south- western part of Nigeria. It is the most populous city in Nigeria and is the center of commercial activities in the country [12]. The survey was administered to registered community pharmacists via the platforms of Association of Community Pharmacists in Nigeria (ACPN) of various local government areas in Lagos state. The ACPN is the technical arm of the Pharmaceutical Society of Nigeria (PSN) committed to empowering every community pharmacist to embrace best pharmacy practice [13]. The study was carried out between February and October, 2021.
Study Design
The study design used for this project was cross sectional study design.
Study Population
The participants involved in the study included licensed pharmacists currently working in a community pharmacy, either as the owner, superintendent pharmacist or as the pharmacist in charge.
Sample Size Techniques
The study involved community pharmacists with a target sample size of 120 respondents conveniently chosen.
Sampling Method
The sampling method used in this study was convenience sampling based on the number of community pharmacists who were willing to participate in the study.
Data Collection Tool
The study was carried out during the pandemic; hence an online questionnaire was used. Data collection tool was created using Google Forms software, an online mobile tool which is used to design customized questionnaires. The questionnaire was structured to cover the main topics:
1. Sociodemographic characteristics including gender, age, position in the pharmacy and number of years in practice.
2. Effect of COVID-19 on the delivery of pharmaceutical care.
3. Effect of COVID-19 on drug availability and prices.A copy of the questionnaire is available in Appendix 1.
Data Collection
The online questionnaire was administered to community pharmacists in Lagos state and their responses were the data source. The questionnaire was sent via the ACPN online platforms as well as other available community pharmacists’ WhatsApp group chats to allow willing pharmacists to participate in the study. The survey was sent out between June and August, 2021, during which daily reminders were sent to get as many responses as possible.
Data Analysis
Data collected was pre-analyzed using the Google Forms software and was further subjected to descriptive statistical analysis using Microsoft Excel software. Descriptive data were presented in tables, bar charts and pie chart. Frequencies and percentages were also used for analysis of data. Comparisons across demographic characteristics were made using Chi square statistics. A probability of 0.05 or less was considered to be significant. For qualitative questions, thematic analysis of responses was performed using appropriate codes.
Ethical Considerations
For this study, ethical approval was obtained from the Health Research Ethics Committee, Lagos University Teaching Hospital (LUTH), Idi-Araba, Lagos, Nigeria, by a Notice of Exemption. The Health Research Committee assigned number was ADM/DCST/ HREC/APP/4167. The pharmacists who participated in filling the questionnaires gave their consent. Utmost confidentiality was ensured during and after data collection.
Results
Consequently, the questionnaires were distributed to one hundred and fifty (150) community pharmacists and one hundred and twenty-five (125) responses were retrieved. The response rate was 83.33%.
Sociodemographic Characteristics
Table 1 shows that from a total of 125 respondents, more than half (56%) were female, and with majority falling within the age range of 25-34 years with the mean age of 32.4 ± 4.7 years. Most of the community pharmacist respondents (67.2%) have been practicing for 0-5 years.
|
SOCIODEMOGRAPHIC CHARACTERISTICS |
FREQUENCY (n=125) |
PERCENTAGE (%) |
|
Gender |
||
|
Female |
70 |
56.0 |
|
Male |
55 |
44.0 |
|
Number of Years in Community Pharmacy Practice (years) |
||
|
0-5 |
84 |
67.2 |
|
6-10 |
12 |
9.6 |
|
11-15 |
11 |
8.8 |
|
16-20 |
5 |
4 |
|
21-25 |
5 |
4 |
|
26-30 |
3 |
2.4 |
|
31-35 |
5 |
4 |
|
Age (years) |
||
|
<25 |
42 |
33.6 |
|
25- 34 |
47 |
37.6 |
|
35- 44 |
18 |
14.4 |
|
45-54 |
10 |
8.0 |
|
55-64 |
7 |
5.6 |
|
>64 |
1 |
0.8 |
|
Mean age = 32.4 ± 4.7 years |
||
Table 1: Sociodemographic Characteristics of Respondents
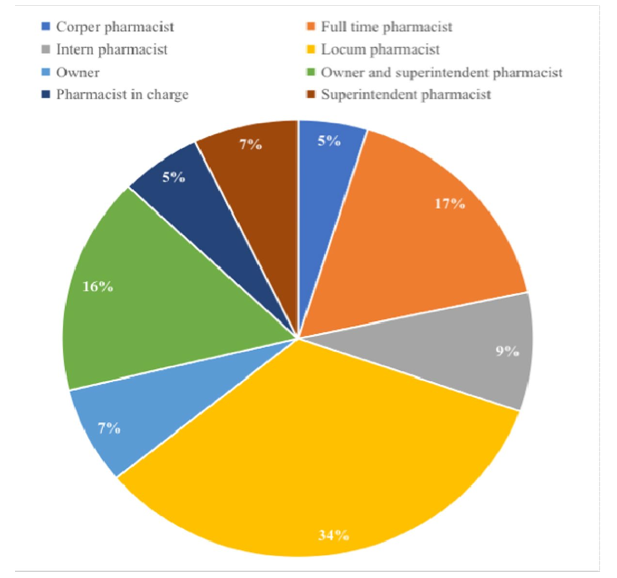
Figure 1: Status of Respondents
Effect of Covid-19 on Delivery of Pharmaceutical Care
The table below shows that the majority of the participants (56%) think there was a total lockdown in the state. Community pharmacies operated during the initial active phase of the pandemic and many (96.8%) of the respondents’ community pharmacies operated during the initial active phase of the pandemic.
|
VARIABLE |
FREQUENCY (n=125) |
PERCENTAGE (%) |
|
The state was on total or partial lockdow |
n |
|
|
No lockdown |
2 |
1.6 |
|
Partial lockdown |
53 |
42.4 |
|
Total lockdown |
70 |
56.0 |
|
Respondent’s community pharmacy operated during the initial active phase of the pandemic |
||
|
Yes |
121 |
96.8 |
|
No |
4 |
3.2 |
Table 2: Community Pharmacy Operation During the Lockdown
Table 3 below shows that most participants practiced the recommended measures to help curb the spread of coronavirus. The most implemented measure was the use of face masks (90.4%). Other commonly practiced measures included restriction in the number of patients for access at a time (90.4%), reduction in number of staff on duty (76.8%) and advice for elderly patients to stay at home (74.4%). Chi square testing against gender and pharmacy status identified that no statistically significant difference exists when compared to the variables.
|
VARIABLE |
YES n (%) |
NO n (%) |
I DON'T KNOW n (%) |
PHARMACY STATUS (LOCUM PHARMACISTS) df; p-value |
GENDER (FEMALE); df; p-value |
|
No face mask, no entry |
113(90.4) |
9(7.2) |
3(2.4) |
1; 0.22 |
1; 0.11 |
|
Restricted number of patients for access at a time |
113(90.4) |
9(7.2) |
3(2.4) |
1; 0.06 |
1; 0.44 |
|
Reduction in the number of staff on duty |
96(76.8) |
25(20) |
4(3.2) |
1; 0.07 |
1; 0.32 |
|
Advice for elderly patients to stay at home |
93(74.4) |
24(19.2) |
8(6.4) |
1; 0.14 |
1; 0.93 |
|
Use of markers to ensure 6 feet distance between patients |
76(60.8) |
46(36.8) |
3(2.4) |
1; 0.28 |
1; 0.76 |
|
Use of glass barriers to create a distance between patients and the counter |
50(40) |
67(54.4) |
7(5.6) |
1; 0.72 |
1; 0.15 |
|
No measures were put in place |
2(1.6) |
114(91.2) |
9(7.2) |
|
|
Table 3: Measures Adopted During Covid-19
Table 4 below shows that the measures adopted during the initial active phase of COVID-19 are still being utilized by some pharmacies and many respondents (68.8%) believe the measures against COVID-19 have affected delivery of pharmaceutical care to patients.
|
VARIABLE |
FREQUENCY (n=125) |
PERCENTAGE (%) |
|
The measures adopted during the pandemic are still being utilized in the operation of your pharmacy |
||
|
Yes |
69 |
55.2 |
|
No |
56 |
44.8 |
|
The measures adopted during the pandemic affect the quality of patient’s care provided in your pharmacy |
||
|
Yes |
86 |
68.8 |
|
No |
19 |
15.2 |
|
I don’t know |
20 |
16.0 |
Table 4: Utilization and Effects of Measures Adopted During the Initial Active Phase of the Pandemic
Figure 2 below shows how the measures implemented have affected the delivery of pharmaceutical care to patients. The top three include decreased time spent with patients during counselling (61.6%), pharmacists no longer checking blood pressure and blood sugar level (40%) increased sales of point of care testing devices (38.4%).

Figure 2: Effect of Covid-19 on the Delivery of Pharmaceutical Care
Table 5 shows that less than half (45.6%) of the respondents believe that the virus has caused moderately positive effects on the pharmaceutical care delivery, while a few of the respondents (32%) believe that there have been moderately negative effects.
|
VARIABLE |
FREQUENCY (n=125) |
PERCEN TAGE (%) |
|
Positive effect of COVID-19 pharmacists on a scale of 1-5 on the delivery of pharmaceutical care by community |
||
|
1 (no effect) |
8 |
6.4 |
|
2 (mildly positive effect) |
15 |
12.0 |
|
3 (moderately positive effect) |
57 |
45.6 |
|
4 (positive effect) |
34 |
27.2 |
|
5 (greatly positive effect) |
11 |
8.8 |
|
Negative effect of COVID-19 pharmacists on a scale of 1-5 on the delivery of pharmaceutical care by community |
||
|
1 (no effect) |
10 |
8.0 |
|
2 (mildly negative effect) |
18 |
14.4 |
|
3 (moderately negative effect) |
40 |
32.0 |
|
4 (negative effect) |
37 |
29.6 |
|
5 (greatly negative effect) |
20 |
16.0 |
Table 5: Rate of Effect of Measures Adopted During the Pandemic on the Patients Care Delivery.
Table 6 shows how respondents have adapted to the changes to ensure delivery of pharmaceutical care. Four thematic areas emerged from respondents on how they ensured the delivery of pharmaceutical care during the pandemic. Many of the respondents ensured the adaptation of the COVID-19 protocols.
|
THEMES |
CODES |
DEFINITION |
|
The pharmacy adapted to these changes to ensure delivery of pharmaceutical care to patients by |
||
|
Adapting to the COVID-19 protocols as recommended by the NCDC |
‘Adapting to protocols’ ‘Implementation of COVID-19 measures’ |
Implementation of COVID-19 measures like the use of face masks, hygiene measures and social distancing. |
|
Referrals to hospitals |
‘Referrals’ |
Referring patients to hospitals for critical cases. |
|
Encouraging tele-pharmacy |
‘Tele-pharmacy’ ‘Calling patients for follow up’ ‘WhatsApp messages’ ‘Online’ |
The use of WhatsApp messages, calls, videos, and text messages to provide education and information and to follow up on patients. |
|
The use of logistics company to offer delivery services for pharmaceutical goods to patients |
‘Home delivery services’ ‘Logistics’ |
Ensuring delivery of medications to clients by the use of logistics especially to elderly patients and ill patients. |
|
EXPLANATORY NOTES THEMES |
||
|
Adapting to the COVID-19 protocols as recommended by the NCDC |
Respondents have ensured the implementation of measures The use of logistics company to of COVID-19 to help limit the spread of the virus. These measures include the use of face masks, hygienic measures and social distancing |
|
|
Referral to hospitals |
Respondents have ensured that they refer patients to clinics in critical cases and also to take the COVID-19 test when they feel the symptoms. |
|
|
Encouraging tele-pharmacy |
Respondents have ensured the use of tele-pharmacy in providing education to patients and in the follow up of patients. The use of logistic services for delivery of medications to elderly patients and ill patients has been implemented by respondents. offer delivery services for pharmaceutical goods to patien |
|
Table 6: How Respondents Ensured the Delivery of Pharmaceutical Care During the Pandemic
Effect of Covid-19 on Drug Availability and Prices
Figure 3 below shows that the COVID-19 has affected the ready availability of medicines in the majority of the respondents’ pharmacies (81.6%).
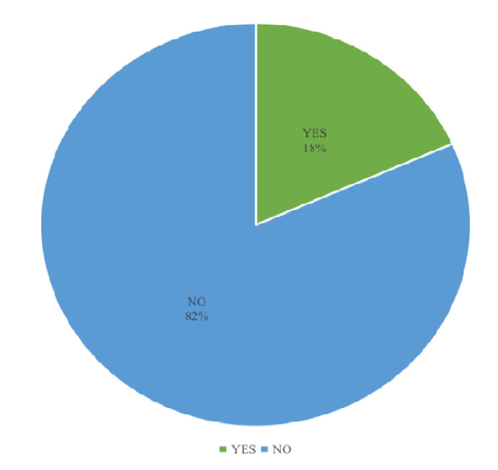
Figure 3: Effect of Covid-19 on the Ready Availability of Medicines in the Pharmacy
Table 7 shows that the most affected class of pharmaceutical products was COVID-19 pharmaceutical goods (53.6%). Others were antimalarials (16.8%), antimicrobials (14.4%) and multivitamins (4.7%).
|
CLASSES AFFECTED OF MEDICINES |
MOST FREQUENCY (n=125) |
PERCENTAGE (%) |
|
COVID-19 pharmaceutical goods (PPE, hand sanitizers, face masks and immune boosters) |
67 |
53.6 |
|
Antimalarials |
21 |
16.8 |
|
Antimicrobials |
18 |
14.4 |
|
Minerals and Vitamins |
6 |
4.7 |
|
Analgesics |
5 |
4.0 |
|
Anti-hypertensive |
3 |
2.4 |
|
Anti-diabetics |
2 |
1.6 |
|
All |
3 |
2.4 |
Table 7: Classes of Medicines Most Affected
The medicines that were in short supply in most of the respondents’ pharmacies include antibiotics (24.8%), immune boosters (18.4%) and hydroxychloroquine (12%).
|
MEDICINES SHORT IN SUPPLY |
FREQUENCY (n=125) |
PERCENTAGE (%) |
|
Antibiotics |
31 |
24.8 |
|
Immune boosters |
23 |
18.4 |
|
Hydroxychloroquine |
15 |
12.0 |
|
Anti-malarial |
5 |
4.0 |
|
Vitamins and Supplements |
2 |
1.6 |
|
Anti-hypertensive |
1 |
0.8 |
|
Analgesics |
1 |
0.8 |
|
Anti-diabetics |
1 |
0.8 |
|
Zinc tablets |
1 |
0.8 |
|
None |
45 |
36.0 |
Table 8: Medicines Short in Supply
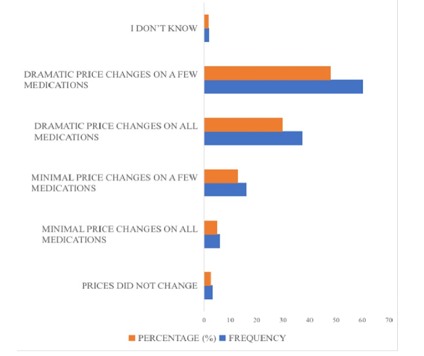
Figure 4: Rating of Price Changes
Table 9 shows that multivitamins and immune boosters had the most dramatic price changes (28.7%). Other medications with dramatic price changes were antimalarials, antibiotics and ivermectin.
|
MEDICINES WITH DRAMATIC PRICE CHANGES |
FREQUENCY (n=125) |
PERCENTAGE (%) |
|
Multivitamins and immune boosters |
53 |
28.7 |
|
Antimalarial |
33 |
17.8 |
|
Antibiotics |
30 |
16.2 |
|
Ivermectin |
27 |
14.6 |
|
Preventive or protective equipment |
12 |
6.5 |
|
Anti-hypertensive |
8 |
4.3 |
|
Antidiabetic |
7 |
3.9 |
|
Antipyretics, antihistamines |
6 |
3.2 |
|
Analgesic |
2 |
1.1 |
|
Infusions and astringent |
2 |
1.1 |
|
Antiviral |
1 |
0.5 |
|
Antifungal |
1 |
0.5 |
|
Asthma drugs |
1 |
0.5 |
|
Imported drugs |
1 |
0.5 |
|
Almost all |
1 |
0.5 |
|
None |
2 |
1.1 |
Table 9: Medicines with Dramatic Price Changes
From Table 10 below, the majority of the respondents (18.4%) were constantly able to contact distributors for supply of drugs during the initial active phase of the pandemic.
|
HOW PATIENTS’ DRUGSUPPLY NEEDS WERE MET |
FREQUENCY (N=125) |
PERCENTAGE (%) |
|
Ask from distributors |
23 |
18.4 |
|
We had enough stock |
17 |
13.6 |
|
Through phone contacts and recommendations |
12 |
9.6 |
|
Bulk purchasing |
18 |
14.4 |
|
Delivery services were introduced and clients paid on delivery |
6 |
4.8 |
|
Better alliance with suppliers |
1 |
0.8 |
|
Tele-pharmacy |
1 |
0.8 |
|
I don’t know |
47 |
37.6 |
Table 10: Ways by which Respondents were Able to Meet Patients’ Drug Supply Needs During the Initial Active Phase of the Pandemic
Discussion
This study was carried out with the aim of assessing the effect of COVID-19 on community pharmacy service delivery. Of 125 participants, 56% were female. This is similar to a study in the Netherlands which had 64.7% female participants [14]. The modal age range was 25-34 years with a mean age of 32.4 ± 4.7 years. This was in contrast with the study in the Netherlands which had a mean age of 43.4 ± 11.5 years [15]. A great percentage of the respondents were locum pharmacists and only few of the respondents were pharmacy owners. This is in contrast to a study carried out in Australia where the majority of the participants were full-time pharmacists and only a few were locum pharmacists [16]. This could be due to the use of online platforms containing more locum pharmacists and less pharmacy owners. Majority of the respondents have had 0-5 years of practice. This is similar to a study carried out in Switzerland in which 79% of the respondents have had <5 years of experience as community pharmacists [17].
The lockdown in Lagos state took effect on March 30, 2020 (Mbah, 2020). Majority of the respondents’ community pharmacies were actively operating during this period. This shows that during the pandemic, community pharmacists were the first point of contact for individuals and they remained accessible to patients, providing health related information and advice [19].
Actions in response to coronavirus were mainly aimed at reducing direct patient contact and limiting the number of patients visiting the pharmacy. The findings show that the measures implemented by the NCDC and CDC were implemented in most community pharmacies. However, there was a variability in the frequency of uptake of some of these measures. For example, the use of face masks, restriction of the number of patients for access at a time, reduction in number of staff on duty and advice for elderly patients to stay at home were implemented by the majority of the pharmacies. The use of glass barriers, however, was less frequently implemented. The study carried out in the Netherlands showed that community pharmacists suggested the use of plastic or glass barriers as a standard for hygiene in the pharmacy [20]. Majority of the community pharmacists ensured the use of face masks in the pharmacy. The use of face masks has been proved to be effective in reducing transmission of the coronavirus (Esposito et al., 2020). More than half of the respondents indicated that the measures are still in use.
The study also reveals that more than half of the pharmacists believed the pandemic has affected the delivery of pharmaceutical care to patients. A good number of the pharmacists believe that the effects have been moderately positive (45.6%) and moderately negative (32%). Majority (61.6%) of the community pharmacists now spend shorter time with patients during counseling. This is in contrast to the study carried out in Australia, where only a few pharmacists found the provision of clinical services and medication counseling challenging [21]. The structural increase in the distance between pharmacists and patients negatively influences patient- pharmacist interaction [22]. Some respondents have had to stop checking blood pressure and blood sugar level. This could also be due to physical distancing.
Decrease in the quality of follow up evaluation has also been noticed. This could be due to the inadequate patient-pharmacist time, physical distancing and advice for elderly patients and ill to stay home. Social and physical distancing may compromise the quality of patient care and medication counseling provided in community pharmacists. However, to ensure the safety of patients and staff, the use of tele-pharmacy has been encouraged [23]. Tele- pharmacy and use of online education tools have been promoted to facilitate communication between pharmacists and their patients [24]. However, only very few of the respondents were able to employ the use of tele-pharmacy and online pharmacy. The methods are difficult because many patients have limited digital skills as well as health literacy and therefore are at risk of drug related problems [25].
Also, the use of logistic procedures to deliver drugs to patients have been implemented. This is essential especially for high risk patients such as elderly patients and critically ill patients [26]. Overall, many of the community pharmacists ensured the practice of the COVID-19 protocols recommended by the NCDC. Majority of the respondents agreed that COVID-19 has affected the ready availability of medicines in their pharmacies. This could be as a result of limited importation of goods from other countries (mainly China and India) and the panic buying practice of customers in response to the pandemic [27]. Also the price increase from pharmaceutical wholesalers and patients buying unnecessary and excessive products have also contributed to the unavailability of some drugs [28]. The COVID-19 pharmaceutical goods were the most affected class of medicines including face masks, sanitizers and preventive or protective equipment (PPE). This is similar to a study conducted in Bangladesh, where over 95% of the stores recorded an increase in the purchase of PPE [29]. Other medicines like antimalarials and antimicrobials were also affected. The antibiotics and immune boosters were short in supply in most pharmacies due to increased demand for them. This is similar to a study carried out in developing countries, where it was shown that there was an increase in utilization of antibiotics and multivitamins in Nigeria, Pakistan, Bangladesh, Ghana and Vietnam [30]. Antimalarials, principally hydroxychloroquine, were also short in supply in some pharmacies (12%). This is also similar to the study carried out in developing countries, where there was an increase in utilization of hydroxychloroquine across most African countries except Namibia [31]. This is as a result of its use as a prophylaxis or treatment of COVID-19 despite the controversies against its usefulness [32].
Findings from this study shows that there were dramatic price changes on a few medicines, especially the immune boosters and antimalarial medicines. This is similar to the study conducted in Bangladesh where dramatic price changes were also noticed. This is as a result of the decrease in importation and increase in utilization during the pandemic [33].
Increase in local production could help address the situation (EAC, 2020).
Conclusion
The research findings reveal that the coronavirus disease 2019 (COVID-19) had considerable impact on the delivery of pharmaceutical care to patients and on the availability of drugs in community pharmacies in Lagos state. Although the lockdown was quite challenging, community pharmacy continued to provide services by implementing measures to reduce the spread of COVID-19. These measures caused a decrease in interaction between pharmacists and their patients. To improve delivery of patient care, pharmacists identified the importance of logistics services and tele-pharmacy in healthcare. Provision of drugs and other pharmaceutical products was challenging, but pharmacists were able to ensure steady delivery of drugs by ensuring bulk purchasing and always contacting suppliers [34-77].
References
- Alexander, G. C., & Qato, D. M. (2020). Ensuring access to medications in the US during the COVID-19 pandemic. Jama, 324(1), 31-32.
- Ozma, M. A., Maroufi, P., Khodadadi, E., Köse, ÃÂ??., Esposito, I., Ganbarov, K., ... & Kafil, H. S. (2020). Clinical manifestation, diagnosis, prevention and control of SARS- CoV-2 (COVID-19) during the outbreak period. Infez Med, 28(2), 153-165.
- Byambasuren, O., Cardona, M., Bell, K., Clark, J., McLaws,M. L., & Glasziou, P. (2020). Estimating the extent of asymptomatic COVID-19 and its potential for community transmission: systematic review and meta-analysis. Oficial Journal of the Association of Medical Microbiology and Infectious Disease Canada, 5(4), 223-234.
- Bergman, S., Cennimo, D. J., Miller, M. M., & Olsen, K. M. (2021). COVID-19 treatment: investigational drugs and other therapies. Medscape, 1-49.
- COVID, C., Team, R., Jorden, M. A., Rudman, S. L., Villarino, E., Hoferka, S., ... & Chung, J. R. (2020). Evidence for limited early spread of COVID-19 within the United States, January– February 2020. Morbidity and Mortality Weekly Report, 69(22), 680.
- WHO Consultative Group on the Role of the Pharmacist in the Health Care System. (1994). The Role of the Pharmacist in the Health Care System: Report of a WHO Consultative Group: New Delhi, 13-16 December 1988; Report of a WHO Meeting: Tokyo, Japan, 31 August-3 September 1993. World Health Organization.
- Hedima, E. W., Adeyemi, M. S., & Ikunaiye, N. Y. (2021). Community Pharmacists: On the frontline of health service against COVID-19 in LMICs. Research in Social and Administrative Pharmacy, 17(1), 1964-1966.
- Hayden, J. C., & Parkin, R. (2020). The challenges of COVID-19 for community pharmacists and opportunities for the future. Irish journal of psychological medicine, 37(3), 198-203.
- CDC Covid-19 Response Team, CDC COVID-19 Response Team, CDC COVID-19 Response Team, Bialek, S., Gierke, R., Hughes, M., ... & Skoff, T. (2020). Coronavirus disease 2019 in children—United States, february 12–april 2, 2020. Morbidity and Mortality Weekly Report, 69(14), 422-426.
- Emanuel, E. J., Persad, G., Upshur, R., Thome, B., Parker, M., Glickman, A., ... & Phillips, J. P. (2020). Fair allocation of scarce medical resources in the time of Covid-19. New England Journal of Medicine, 382(21), 2049-2055.
- Li, Q. (2020). An outbreak of NCIP (2019-nCoV) infection in China—wuhan, Hubei province, 2019− 2020. China CDC Weekly, 2(5), 79.
- Campbell, J. (2012). This is Africa’s new biggest city. Council on Foreign Relations blog Cennimo, D. J. (2021) Coronavirus Disease 2019 (COVID-19).
- Ajibola, O. G. (2024). An Assessment of the Effects of Coronavirus Disease 2019 (COVID-19) on Community Pharmacy Service Delivery in Lagos State. medRxiv, 2024-11.
- Koster, E. S., Philbert, D., & Bouvy, M. L. (2015). Healthliteracy among pharmacy visitors in the Netherlands.Pharmacoepidemiology and drug Safety, 24(7), 716-721.
- Koster, E. S., Philbert, D., & Bouvy, M. L. (2021). Impact of the COVID-19 epidemic on the provision of pharmaceutical care in community pharmacies. Research in Social and Administrative Pharmacy, 17(1), 2002-2004.
- Sum, Z. Z., & Ow, C. J. (2021). Community pharmacy response to infection control during COVID-19. A cross- sectional survey. Research in Social and Administrative pharmacy, 17(1), 1845-1852.
- Hoti, K., Jakupi, A., Hetemi, D., Raka, D., Hughes, J., & Desselle, S. (2020). Provision of community pharmacy services during COVID-19 pandemic: a cross sectional study of community pharmacists’ experiences with preventative measures and sources of information. International journal of clinical pharmacy, 42, 1197-1206.
- Mbah, F. (2020). Nigeria announces lockdown of major citiesto curb coronavirus. Retrieved online June, 8, 2020.
- Secretariat, E. A. C. (2020). East African community Covid-19response plan. Arusha: East African community.
- Esposito, S., Principi, N., Leung, C. C., & Migliori, G.B. (2020). Universal use of face masks for success against COVID-19: evidence and implications for prevention policies. European Respiratory Journal, 55(6).
- Gallegos, A. (2020). WHO declares public health emergency for novel coronavirus. Medscape Medical News, 30(1).
- Liu, S., Luo, P., Tang, M., Hu, Q., Polidoro, J. P., Sun, S., & Gong, Z. (2020). Providing pharmacy services during the coronavirus pandemic. International journal of clinical pharmacy, 42, 299-304.
- Uwizeyimana, T., Hashim, H. T., Kabakambira, J. D., Mujyarugamba, J. C., Dushime, J., Ntacyabukura, B., ... & Lucero-Prisno, D. E. (2021). Drug supply situation in Rwanda during COVID-19: issues, efforts and challenges. Journal of Pharmaceutical Policy and Practice, 14, 1-4.
- Haque, M., Islam, S., Iqbal, S., Urmi, U. L., Kamal, Z. M., Shuvo, S. A., ... & Godman, B. (2020). Availability and price changes of potential medicines and equipment for the prevention and treatment of COVID-19 among pharmacy and drug stores in Bangladesh; findings and implications. Bangladesh Journal of Medical Science, 19, S36-S50.
- Sefah, I. A., Ogunleye, O. O., Essah, D. O., Opanga, S. A.,Butt, N., Wamaitha, A., ... & Godman, B. (2021). Rapid assessment of the potential paucity and price increases for suggested medicines and protection equipment for COVID-19 across developing countries with a particular focus on Africa and the implications. Frontiers in pharmacology, 11, 588106.
- Edara, V. V., Pinsky, B. A., Suthar, M. S., Lai, L., Davis- Gardner, M. E., Floyd, K., ... & Fabrizio, T. P. (2021). Infection and vaccine-induced neutralizing-antibody responses to the SARS-CoV-2 B. 1.617 variants. New England Journal of Medicine, 385(7), 664-666.
- Li, G., Li, W., He, X., & Cao, Y. (2020). Asymptomatic and presymptomatic infectors: hidden sources of coronavirus disease 2019 (COVID-19). Clinical Infectious Diseases, 71(8), 2018-2018.
- Olafenwa, B. R. (2021). COVID-19 as a public health problem in Nigeria: A sociopragmatic reading of health issues in Jenifa on Lockdown. In Proceeding of the International Conference on Arts and Humanities (Vol. 8, No. 01, pp. 11-24).
- Bluml, B. M., Watson, L. L., Skelton, J. B., Manolakis, P. G., & Brock, K. A. (2014). Improving outcomes for diverse populations disproportionately affected by diabetes: Final results of Project IMPACT: Diabetes. Journal of the American Pharmacists Association, 54(5), 477-485.
- Brodie, D. C. (1981). Pharmacy's societal purpose. Americanjournal of hospital pharmacy, 38(12), 1893-1896.
- Rothholz, M. C. (2013). The role of community pharmacies/pharmacists in vaccine deliver in the United States.
- Cherian, S., Potdar, V., Jadhav, S., Yadav, P., Gupta, N., Das, M., ... & INSACOG Consortium. (2021). Convergent evolution of SARS-CoV-2 spike mutations, L452R, E484Q and P681R, in the second wave of COVID-19 in Maharashtra, India. BioRxiv, 2021-04.
- Strand, L. M., Cipolle, R. J., Morley, P. C., & Frakes, M. J. (2004). The impact of pharmaceutical care practice on the practitioner and the patient in the ambulatory practice setting: twenty-five years of experience. Current pharmaceutical design, 10(31), 3987-4001.
- Ajibola, O. G. (2024). An Assessment of the Effects of Coronavirus Disease 2019 (COVID-19) on Community Pharmacy Service Delivery in Lagos State. medRxiv, 2024-11.
- Cassidy, C., Dever, D., Stanbery, L., Edelman, G., Dworkin, L., & Nemunaitis, J. (2020). FDA efficiency for approval process of COVID-19 therapeutics. Infectious Agents and Cancer, 15, 1-13.
- Goode, J. V. R., Owen, J. A., Bennett, M. S., & Burns, A.L. (2019). A marathon, not a sprint: Growth and evolution of communityâ?ÂÂbased pharmacy residency education and training. Journal of the American College of Clinical Pharmacy, 2(4), 402-413.
- Hepler, C. D., & Strand, L. M. (1990). Opportunities and responsibilities in pharmaceutical care. American journal of hospital pharmacy, 47(3), 533-543.
- Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., ... &Cao, B. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet, 395(10223), 497-506.
- Ibrahim, R. L., Ajide, K. B., & Julius, O. O. (2020). Easing of lockdown measures in Nigeria: Implications for the healthcare system. Health policy and technology, 9(4), 399-404.
- Joda, A. E., Olugbake, O. A., Oyetunde, O. O., Awofisayo, O., Ibrahim, M. B., Williams, F. E., ... & Ologunagba, M. O. (2020). Pharmacists’ perception of their roles and involvement in coronavirus disease 2019 (COVID-19).
- Lauer, S. A., Grantz, K. H., Bi, Q., Jones, F. K., Zheng, Q., Meredith, H. R., ... & Lessler, J. (2020). The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Annals of internal medicine, 172(9), 577-582.
- Mikeal, R. L., Lazarus, H. L., Vinson, M. C., & Brown, T. R. (1975). Quality of pharmaceutical care in hospitals. American Journal of Health-System Pharmacy, 32(6), 567-574.
- Auwal, S. G., Abubakar, S. A., Mustapha, M. T., & Shehu, S.U. (2020). COVID-19 Pandemic in Nigeria: A review of the first three months. International Journal of Public Health and Clinical Sciences, 7(4), 32-41.
- Danguguwa, K. I. (2020). NATIONAL RESPONSE STRATEGY AND INTERNATIONAL SUPPORT IN FIGHTING COVID-19 IN IDPS CAMPS IN NORTHEAST NIGERIA. EDITORS/REVIEWERS.
- Ajibola, O. G. (2024). An Assessment of the Effects of Coronavirus Disease 2019 (COVID-19) on Community Pharmacy Service Delivery in Lagos State. medRxiv, 2024-11.
- Auwal, S. G., Abubakar, S. A., Mustapha, M. T., & Shehu, S.U. (2020). COVID-19 Pandemic in Nigeria: A review of the first three months. International Journal of Public Health and Clinical Sciences, 7(4), 32-41.
- Ajibola, O. G. (2024). An Assessment of the Effects of Coronavirus Disease 2019 (COVID-19) on Community Pharmacy Service Delivery in Lagos State. medRxiv, 2024-11.
- Al-Shattarat, B., & Amuda, Y. J. (2021). Comparative report of compliance to precautionary measures against COVID-19 in Nigeria and Jordan. Heliyon, 7(8).
- Anazonwu, N. P., Nnamani, K. E., Osadebe, N., Anichebe, O., Ezeibe, C. C., Mbah, P. O., & Nzeadibe, T. C. (2022). State actors, human rights violations and informal livelihoods during the COVID-19 pandemic in Nigeria. Territory, politics, governance, 10(6), 876-895.
- Ajibola, O. G. (2024). An Assessment of the Effects of Coronavirus Disease 2019 (COVID-19) on Community Pharmacy Service Delivery in Lagos State. medRxiv, 2024-11.
- Ajibola, O. G. (2024). An Assessment of the Effects of Coronavirus Disease 2019 (COVID-19) on Community Pharmacy Service Delivery in Lagos State. medRxiv, 2024-11.
- Oladipo, E. K., Ajayi, A. F., Odeyemi, A. N., Akindiya,O. E., Adebayo, E. T., Oguntomi, A. S., ... & Oloke, J. K. (2020). Laboratory diagnosis of COVID-19 in Africa: availability, challenges and implications. Drug Discoveries & Therapeutics, 14(4), 153-160.
- Omilana, T. (2020). Buhari extends phase two of COVID-19 lockdown by four weeks.
- Ong, S. W. X., Tan, Y. K., Chia, P. Y., Lee, T. H., Ng, O. T., Wong,M. S. Y., & Marimuthu, K. (2020). Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. Jama, 323(16), 1610-1612.
- Obitube, K., Ajaero, I. D., & Odeh, B. (2023). Timing and effectiveness of media frames reporting the COVID-19 pandemic in Nigeria. Southern African Linguistics and Applied Language Studies, 41(4), 479-495.
- Oran, D. P., & Topol, E. J. (2020). Prevalence of asymptomatic SARS-CoV-2 infection: a narrative review. Annals of internal medicine, 173(5), 362-367.
- Obitube, K., Ajaero, I. D., & Odeh, B. (2023). Timing and effectiveness of media frames reporting the COVID-19 pandemic in Nigeria. Southern African Linguistics and Applied Language Studies, 41(4), 479-495.
- Udochu, E., & Malematja, S. (2023). The Politics of Quarantine and Nigeria’s National Security. African Perspectives on Global Pandemics and the Challenges of Peace and Security, 67.
- Dopp, A. L., Fitall, E., Hall, K. K., & Gale, B. (2020). Health Care Delivery and Pharmacists During the COVID-19 Pandemic. Oncology Practice Management, 10(9).
- Rabin, R. C. (2020). Lost sense of smell may be peculiar clue to coronavirus infection. The New York Times, 26(03), 2020.
- Spinato, G., Fabbris, C., Polesel, J., Cazzador, D., Borsetto, D., Hopkins, C., & Boscolo-Rizzo, P. (2020). Alterations in smell or taste in mildly symptomatic outpatients with SARS- CoV-2 infection. Jama, 323(20), 2089-2090.
- Oyeranti, O., & Sokeye, B. (2020). The evolution and spread of Covid-19 in Nigeria. Centre for Petroleum, Energy Economics and Law (CPEEL), 1-18.
- Nigeria, U. N. I. C. E. F. (2021). COVID-19 vaccines shippedby COVAX arrive in Nigeria.
- Visscher, B. B., Steunenberg, B., Heerdink, E. R., & Rademakers, J. (2020). Medication self-management support for people with diabetes and low health literacy: a needs assessment. PLoS One, 15(4), e0232022.
- World Health Organization. (2014). Infection prevention and control of epidemic-and pandemic-prone acute respiratory infections in health care. World Health Organization
- WHO, W. (2020). Novel Coronavirus (2019-nCoV) Situation Report—1. who.
- WHO. (2020). World Health Organization Coronavirusdisease (COVID-19). Situation Report-189.
- World Health Organization. (2021). Infection prevention and control during health care when coronavirus disease (COVID-19) is suspected or confirmed: interim guidance, 12 July 2021 (No. WHO/2019-nCoV/IPC/2021.1). World Health Organization.
- World Health Organization. (2020). COVID-19 weeklepidemiological update, 3 November 2020.
- World Health Organization. (2020). Coronavirus disease 2019 (COVID-19): situation report, 73.
- WHO, E. R. V. (2020). Including COVID-19: Methods for Detection. World Health Organization, Geneva, Switzerland.
- Director-General, W. H. O. (2020). WHO director-general’s opening remarks at the media briefing on COVID-19. World Health Organization.
- World Health Organization. (2020). Strengthening the health systems response to COVID-19: technical guidance# 6: preventing and managing the COVID-19 (No. WHO/ EURO: 2020-804-40539-54460). World Health Organization. Regional Office for Europe.
- Isah, M. B., Abdulsalam, M., Bello, A., Ibrahim, M. I., Usman, A., Nasir, A., ... & Nass, S. S. (2020). Corona Virus Disease 2019 (COVID-19): Knowledge, attitudes, practices (KAP) and misconceptions in the general population of Katsina State, Nigeria. MedRxiv, 2020-06.
- Wiedenmayer, K., Summers, R. S., Mackie, C. A., Gous, A.G., Everard, M., Tromp, D., & World Health Organization. (2006). Developing pharmacy practice: a focus on patient care: handbook (No. WHO/PSM/PAR/2006.5). World Health Organization.
- Williamson, E. J., Walker, A. J., Bhaskaran, K., Bacon, S., Bates, C., Morton, C. E., ... & Goldacre, B. (2020). Factors associated with COVID-19-related death using OpenSAFELYNature, 584(7821), 430-436.
- Wu, Z., & McGoogan, J. M. (2020). Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. jama, 323(13), 1239-1242.