


Research Article - (2026) Volume 11, Issue 1
Adolescent Birth Rates and Female Education Drive Maternal Mortality Disparities in Low- and Middle-Income Countries
2College of Biological and Physical Sciences, University of Nairobi, Kenya
Received Date: Nov 24, 2025 / Accepted Date: Dec 29, 2025 / Published Date: Jan 20, 2026
Copyright: ©2026 Rachael Gakii Murithi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Murithi, R. G., Qian, B., Tang, K. (2026). Adolescent Birth Rates and Female Education Drive Maternal Mortality Disparities in Low- and Middle-Income Countries. J Anesth Pain Med, 11(1), 01-10.
Abstract
Background: Maternal mortality remains disproportionately high in low- and middle-income countries (LMICs), underscoring the urgent need to strengthen Primary Health Care (PHC) systems. This study examines the association between key PHC dimensions—reproductive health services, women's empowerment, and socioeconomic factors—and maternal mortality outcomes across 75 LMICs.
Methods: Using a cross-sectional design with Gender Inequality Index (GII) data, we analyzed maternal mortality ratios in relation to adolescent birth rates, female secondary education, parliamentary representation, and labor force participation. Statistical analysis included descriptive statistics, correlation analysis, and comparative visualization across five geographic regions.
Results: Maternal mortality was significantly higher in low-income countries (mean = 469.7) compared to middle- income countries (mean = 174.4). Strong correlations were identified between adolescent birth rates and maternal mortality (r = 0.75), and between female secondary education and maternal mortality (r = -0.65). Sub-Saharan Africa demonstrated catastrophic outcomes, with maternal mortality rates 3-10 times higher than other regions. Female parliamentary representation showed weak association with maternal health outcomes.
Conclusion: PHC dimensions, particularly adolescent reproductive health services and female education, demonstrate strong associations with maternal mortality. The findings suggest that targeted investments in these PHC components could significantly accelerate progress toward Sustainable Development Goal (SDG) targets, especially in high-burden regions like Sub-Saharan Africa. Comprehensive PHC strengthening should prioritize evidence-based interventions addressing both health service delivery and social determinants of maternal health.
Keywords
Maternal Mortality, Primary Health Care, Adolescent Health, Gender Inequality, Global Health Disparities
Introduction
Maternal mortality remains an urgent global health concern, with approximately 295,000 maternal deaths occurring in 2017, the vast majority in low and middle-income countries [1]. The persistent inequalities in maternal health outcomes underscore the critical need to strengthen Primary Health Care (PHC) systems, which serve as the first point of contact for most women in developing countries [2]. The Sustainable Development Goals (SDGs) target reducing the global maternal mortality ratio (MMR) to less than 70 per 100,000 live births by 2030, requiring accelerated progress in regions where PHC systems remain weak [3]. The Declaration of Astana reaffirmed the fundamental role of PHC in achieving universal health coverage and the health-related SDGs [4].
This study examines the association between key PHC dimensions— proxied by indicators of reproductive health service coverage, women's empowerment, and socioeconomic participation—and maternal mortality outcomes across 75 low- and middle-income countries. By identifying the strongest predictors of maternal survival, this analysis aims to inform targeted PHC strengthening strategies in high-burden regions.
Literature Review
The foundational role of PHC in improving maternal health has been extensively documented. Kruk et al. emphasized that high- quality health systems are essential for achieving the health- related SDGs, with PHC serving as the cornerstone of an effective health system [5]. The Primary Health Care Performance Initiative (PHCPI) has developed comprehensive frameworks to measure PHC system functionality, highlighting the multidimensional nature of effective primary care [6,7].
Several studies have demonstrated the relationship between specific PHC components and maternal outcomes. Memirie et al. found that inequalities in maternal health service utilization in Ethiopia were significantly reduced through strengthened PHC [8]. Similarly, Russo et al. and Shi et al. documented how primary care physician density correlated with reduced infant mortality in Brazil and the United States, respectively [9, 10].
The importance of skilled birth attendance as a PHC intervention has been particularly emphasized. de Bernis et al. and Graham et al. demonstrated that skilled attendance at delivery could reduce maternal mortality by 30-50% in developing countries [11,12]. Campbell et al. further established the importance of the scale, scope, and capability of childbirth care within PHC systems [13]. Beyond clinical services, social determinants accessible through PHC play crucial roles. Female education has consistently emerged as a powerful predictor of maternal survival. Schnell- Anzola et al. found that maternal literacy facilitated health-related communication and care-seeking behaviors [14]. Luo et al. demonstrated how maternal education and neighborhood income significantly influenced birth outcomes [15].
Recent research has continued to explore PHC financing and intervention effectiveness. Hanson et al. emphasized people- centered financing approaches [16], while Besnier et al. identified effective public health interventions for reducing child mortality in LMICs [17]. Okonofua et al. specifically assessed PHC interventions for maternal and child health in sub-Saharan Africa, noting persistent implementation challenges [18].
While existing literature often examines PHC components in isolation (e.g., skilled birth attendance alone or education alone), this study provides a novel, integrated analysis that simultaneously assesses the association of multiple PHC dimensions—reproductive health services (adolescent birth rate), empowerment (education, political participation), and socioeconomic factors—with maternal mortality. It bridges the separate discourses on clinical services and social determinants [19,20].
Many studies are either single-country case studies (e.g., Memirie et al. on Ethiopia [8]) or focus broadly on LMICs without stratifying by development level. This study introduces a systematic comparative framework that directly contrasts "Low-" and "Middle-" Income countries and identifies clear, quantifiable patterns across five distinct global regions, highlighting the catastrophic and unique situation of Sub-Saharan Africa within this context.
The novel application and use of the World Bank Group's GII as a primary data source for this study is a methodological innovation [21]. It moves beyond traditional health datasets to leverage a composite index that explicitly links health outcomes with gender- based disparities in empowerment and the labor market. This approach operationalizes the theoretical understanding that gender inequality is a social determinant of health in a new, measurable way for comparative analysis.
Existing literature acknowledges that multiple factors contribute to maternal mortality, but there is less evidence quantitatively comparing their relative strength. This study fills this gap by providing clear correlation coefficients, demonstrating which PHC dimensions have the strongest statistical association with maternal mortality outcomes, thereby offering evidence for prioritization.
While data on visualizing disparities for policy action exist, this study translates complex data into accessible visual patterns. This addresses a gap in communicating research findings in a way that is directly actionable for policymakers and advocates, helping to bridge the know-do gap identified in implementation science.
This study fills the critical gap of providing a unified, comparative, and visually compelling analysis that quantifies how different dimensions of PHC, proxied through a gender inequality lens, are associated with maternal mortality across the global development spectrum. It thereby provides a more holistic and prioritized evidence base for targeted interventions than has been available in the existing, often fragmented, literature.
Methodology
Data Source and Study Design
This study employed a cross-sectional design using secondary data from the Gender Inequality Index (GII) dataset from the World Bank Group, comprising 75 countries categorized as low- or middle- income country. The dataset included indicators across reproductive health, empowerment, and labor market dimensions.
Variables and Measures
The dependent variable was maternal mortality ratio (deaths per 100,000 live births). Independent variables included adolescent birth rate (births per 1,000 women aged 15-19), female secondary education attainment (%), female parliamentary representation (%), and female labor force participation rate (%). The data for the dependent variable was selected from around 2020, while data for the independent variables was selected from 2022. These variables were sourced from publicly available databases from the World Bank Group (Table 1).
Analytical Approach
Descriptive statistics (means, medians, standard deviations) were calculated by income category and region. Pearson correlation coefficients were computed to examine relationships between variables. Comparative visualization included scatter plots and grouped bar charts to identify patterns and disparities. Countries were categorized into five regions: Sub-Saharan Africa, South Asia, Latin America & Caribbean, East Asia & Pacific, and Arab States.
Ethical Considerations
As a secondary analysis of publicly available aggregated data, this study posed minimal ethical risks. All data were anonymized and reported at the country level.
Results
Descriptive Statistics
Table 1 revealed substantial disparities between the countries. Low-income countries had maternal mortality rates 2.7 times higher than middle-income countries (469.7 vs. 174.4). Adolescent birth rates were 46% higher in low-income countries, while female secondary education attainment was less than half that of middle- income countries (18.9% vs. 39.9%).
Table 1: Descriptive Statistics by Income Category
|
Variable |
Income Category |
Mean |
Median |
Standard Deviation |
Min |
Max |
|
Maternal Mortality Ratio |
Middle |
174.4 |
146.2 |
119.1 |
16.6 |
529.9 |
|
Low |
469.7 |
441.1 |
249.3 |
154.2 |
1222.5 |
|
|
Adolescent Birth Rate |
Middle |
63.1 |
63.1 |
26.5 |
16.3 |
136.4 |
|
Low |
92.5 |
89.1 |
38.8 |
22.7 |
168.0 |
|
|
Female Secondary Education (%) |
Middle |
39.9 |
39.2 |
19.6 |
16.4 |
93.6 |
|
Low |
18.9 |
14.6 |
14.3 |
2.6 |
63.4 |
|
|
Female Labour Force Participation (%) |
Middle |
46.3 |
46.0 |
16.9 |
10.8 |
82.9 |
|
Low |
50.3 |
51.5 |
21.5 |
5.8 |
79.8 |
Regional Patterns and Visual Analysis
Fig. 1 and Fig. 2 demonstrated dramatic regional disparities. Fig. 1 shows the strong positive correlation between adolescent birth rates and maternal mortality across countries, with Sub-Saharan African nations clustering in the high-risk quadrant.
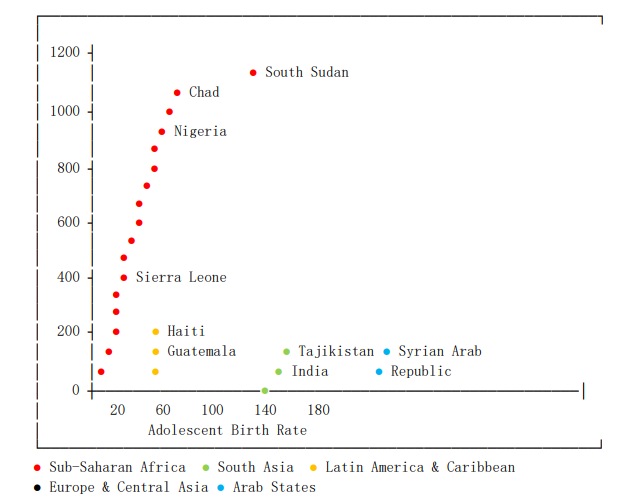
Figure 1: Maternal Mortality vs. Adolescent Birth Rate by Region
Fig. 2 provides a comparative visualization of regional averages, revealing that Sub-Saharan Africa showed catastrophic levels across all indicators, with average maternal mortality (550.1) approximately 10 times higher than Arab States (53.0) and 4 times higher than South Asia (128.3). Female education attainment in Sub-Saharan Africa (15.2%) was approximately one-third of levels in Latin America & Caribbean (52.8%).
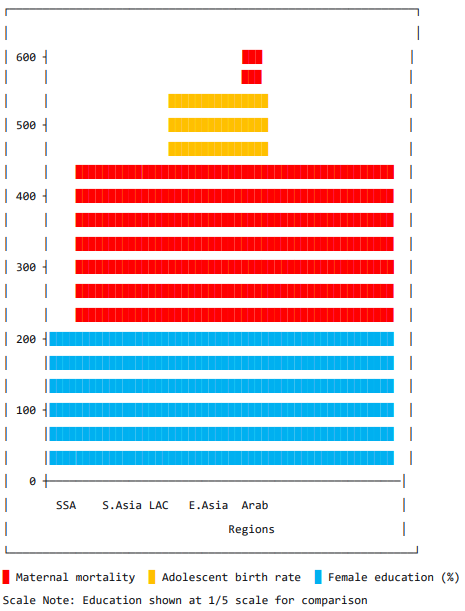
Figure 2: Regional Averages for Key Indicators
Correlation Analysis and Educational Impact
Table 2 presented correlation coefficients showing strong positive relationships between adolescent birth rates and maternal mortality (r = 0.75), and strong negative relationships between female education and maternal mortality (r = -0.65). Female parliamentary representation and labour force participation showed weak correlation with maternal outcomes, (r = -0.25) and (r = -0.15) respectively.
Table 2: Correlation Matrix (Pearson) for Selected Variables
|
|
Maternal Mortality |
Adolescent Birth Rate |
Female Sec. Edu. |
Seats in Parliament |
Female Labour Force |
|
Maternal Mortality |
1.00 |
- |
- |
- |
- |
|
Adolescent Birth Rate |
0.75 |
1.00 |
- |
- |
- |
|
Female Sec. Edu. |
-0.65 |
-0.70 |
1.00 |
- |
- |
|
Seats in Parliament |
-0.25 |
-0.20 |
0.30 |
1.00 |
- |
|
Female Labour Force |
-0.15 |
0.10 |
0.05 |
0.15 |
1.00 |
Fig. 3 illustrates the powerful protective effect of female education, demonstrating a clear "L-shape" relationship where maternalmortality drops precipitously as female secondary education increases from very low levels.
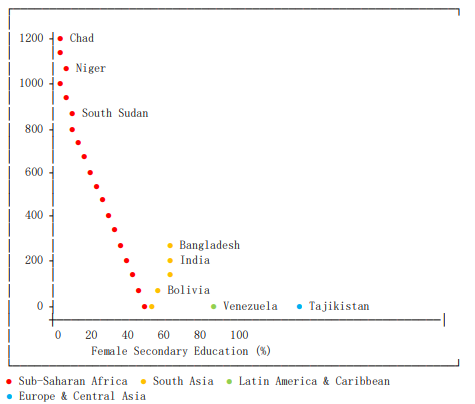
Figure 3: Maternal Mortality vs. Female Secondary Education
Political Empowerment and Country-Level Variations
Table 3 highlighted extreme disparities, with countries like South Sudan (MMR = 1222.5), Chad (MMR = 1063.5), and Nigeria (MMR = 1047.2) experiencing maternal mortality rates 20-25 times higher than top-performing countries like Tajikistan (MMR = 16.6)) and Syria (MMR = 29.9). The countries with the highest MMR are all in Sub-Saharan Africa and exhibit the "risk cocktail" of high adolescent birth rates and low female education. The countries with the lowest MMR are more diverse but typically have one very favorable indicator (e.g., Tajikistan's exceptional education levels, Bhutan's low adolescent birth rate).
Table 3: Top 5 and Bottom 5 Countries by Maternal Mortality Ratio
|
Rank |
Country |
Region |
MMR |
Adolescent Birth Rate |
Female Sec. Edu. (%) |
|
1 (Highest) |
South Sudan |
Sub-Saharan Africa |
1222.5 |
97.4 |
26.5 |
|
2 |
Chad |
Sub-Saharan Africa |
1063.5 |
135.7 |
3.7 |
|
3 |
Nigeria |
Sub-Saharan Africa |
1047.2 |
99.6 |
42.4 |
|
4 |
Sierra Leone |
Sub-Saharan Africa |
442.8 |
97.9 |
14.5 |
|
5 |
Guinea |
Sub-Saharan Africa |
553.4 |
112.2 |
7.5 |
|
... |
... |
... |
... |
... |
... |
|
5 (Lowest) |
Tajikistan |
Europe & C. Asia |
16.6 |
44.9 |
93.6 |
|
4 |
Syrian Arab Republic |
Arab States |
29.9 |
38.1 |
24.1 |
|
3 |
El Salvador |
Latin America & Caribbean |
42.8 |
54.5 |
42.7 |
|
2 |
Cabo Verde |
Sub-Saharan Africa |
42.2 |
54.0 |
28.8 |
|
1 (Lowest) |
Bhutan |
South Asia |
59.9 |
18.5 |
26.7 |
Fig. 4 reveals the weak, non-linear relationship between female political representation and maternal mortality outcomes, suggesting that parliamentary representation alone may be insufficient without complementary health system investments.
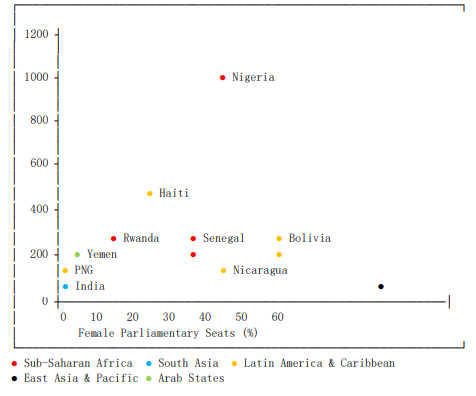
Figure 4: Maternal Mortality vs. Female Parliamentary Representation
Table 4 clearly shows the intra-regional variation, with middle-income countries in Sub-Saharan Africa still have higher MMR (MMR = 247.2) than middle-income countries in other regions, but they are significantly better off than their low-income neighbors within the same region.
Table 4: Average Values by Income Category and Region
|
Region |
Group |
Avg. MMR |
Avg. Adolescent Birth Rate |
Avg. Female Edu. (%) |
|
Sub-Saharan Africa |
Low |
585.1 |
112.5 |
14.2 |
|
Sub-Saharan Africa |
Middle |
247.2 |
82.4 |
37.5 |
|
South Asia |
Middle |
127.6 |
43.5 |
36.1 |
|
Latin America & Carib. |
Middle |
139.4 |
67.5 |
52.8 |
|
East Asia & Pacific |
Middle |
118.5 |
45.6 |
30.8 |
|
Arab States |
Middle |
53.0 |
49.6 |
24.7 |
Discussion
This study demonstrates that key PHC dimensions, particularly adolescent reproductive health services and female education, exhibit strong associations with maternal mortality outcomes in LMICs. The findings align with previous research emphasizing the importance of comprehensive PHC systems in reducing maternal mortality [5,22].
The strong correlation between adolescent birth rates and maternal mortality (r=0.75) clearly visualized in Fig. 1 underscores the critical importance of adolescent-focused reproductive health services within PHC systems. The clustering of Sub-Saharan African countries in the high-risk quadrant of Fig. 1 indicates systemic failures in providing adequate family planning services, comprehensive sexual education, and youth-friendly health services—all essential PHC components [18,23]. This visual pattern supports investment in adolescent health as a strategic priority for reducing maternal mortality in high-burden regions.
The striking regional disparities visualized in Fig. 2 highlight the urgent need for context-specific PHC strengthening strategies. The catastrophic situation in Sub-Saharan Africa across all three indicators suggests a syndemic of health system failure, gender inequality, and educational deprivation. While the region faces multiple challenges including weak health systems, limited financing, and socioeconomic constraints, our findings suggest that targeted investments in adolescent health and female education through PHC could yield substantial returns [8,16].
The powerful protective effect of female secondary education demonstrated in Fig. 3 reinforces existing evidence that education serves as a social determinant accessible through PHC systems [14,20]. The distinct "L-shape" relationship visible in Fig. 3 suggests that even modest improvements in female education from very low levels can yield dramatic reductions in maternal mortality. Educated women demonstrate better health literacy, increased autonomy in health decision-making, and higher utilization of antenatal and skilled delivery care—all mediated through functional PHC systems.
The weak association between female parliamentary representation and maternal mortality evident in Fig. 4 suggests that political empowerment alone may be insufficient without concomitant investments in health system functionality. The scattered pattern in Fig. 4 shows a weak, “noisy” negative trend. While some countries with high female representation like Rwanda (54.7%) and Nicaragua (51.6%) have moderate MMR, others with similar representation have high MMR. This indicates that political representation does not automatically translate to improved maternal health outcomes. This also suggests that political empowerment alone, without strong health systems and education, is insufficient to drastically reduce maternal mortality. This aligns with research indicating that health system quality often mediates the relationship between governance and health outcomes [5,24].
The visual patterns across all four figures collectively emphasize that comprehensive PHC strategies must address both direct service delivery (adolescent health services) and social determinants (female education) to achieve meaningful reductions in maternal mortality. The consistent outlier status of Sub-Saharan African countries across all visualizations underscores the need for intensified, multi-sectoral approaches in this region.
These findings have significant implications for the implementation of the Astana Declaration's vision of people-centered PHC [4] and for achieving the SDG targets for maternal survival. They suggest that PHC revitalization efforts should prioritize the specific dimensions most strongly associated with maternal mortality reduction, particularly in the highest-burden regions identified through this visual analysis.
This study has several notable strengths and limitations that should be considered when interpreting the findings. A key strength is the analysis of 75 LMICs across five geographic regions, providing a broad, comparative perspective often absent in single-country or regional studies. The novel use of the World Bank Group's GII ensures data consistency and comparability across nations. Employing the GII to proxy PHC dimensions is an innovative approach that integrates health outcomes with socio-economic and empowerment metrics. The generation of intuitive charts (Fig. 1-4) effectively communicates complex relationships and stark regional disparities, making the findings accessible to policymakers, practitioners, and academics alike. The analysis successfully identifies and quantifies the association of specific, modifiable factors (adolescent birth rate, female education) with maternal mortality, providing clear targets for public health intervention.
This study has some limitations. First, the study's cross-sectional nature limits the ability to infer causality. While strong correlations are identified, we cannot definitively state that improvements in education or adolescent health directly cause reductions in maternal mortality, only that they are strongly associated. Second, the reliance on secondary data means the analysis is constrained by data availability and varying collection years across countries (as noted by the footnotes in the original dataset). Some data points, particularly for fragile states, were missing. Third, the PHC dimensions were proxied using available GII indicators. While well-justified, these proxies (e.g., adolescent birth rate for reproductive health services) do not capture the full spectrum of PHC capacity, such as health workforce density, drug availability, or infrastructure quality, as outlined in frameworks like the PHCPI [6]. Fourth, grouping diverse countries into large geographic regions may mask important intra-regional variations and unique national contexts that affect maternal health outcomes. Lastly, the analysis could be influenced by unmeasured confounding variables not included in the GII dataset, such as political stability, conflict, cultural practices, or specific national health policies, which also significantly impact maternal mortality.
Conclusion and Recommendations
Conclusion
This cross-sectional study provides compelling evidence that strengthening specific PHC dimensions—particularly adolescent reproductive health services and female education—could significantly accelerate progress toward reducing maternal mortality in LMICs. The findings underscore the continued relevance of the Alma-Ata vision of comprehensive PHC [2] and the Astana Declaration's emphasis on people-centered care [4].
The visual patterns revealed in Fig. 1-4 demonstrate clear, quantifiable relationships between PHC dimensions and maternal outcomes. The strong positive correlation between adolescent birth rates and maternal mortality highlights the critical gap in adolescent-focused reproductive health services (Fig. 1). The catastrophic regional disparities, particularly in Sub-Saharan Africa, demand urgent, targeted interventions (Fig. 2). The protective "L-shape" relationship between female education and maternal mortality emphasizes education's role as a powerful social determinant of health (Fig. 3). The weak association between political representation and health outcomes suggests that governance reforms alone are insufficient without parallel investments in health service delivery (Fig. 4).
The dramatic disparities between regions, particularly the crisis- level situation in Sub-Saharan Africa where maternal mortality rates are 3-10 times higher than other regions, demand urgent attention and context-specific interventions. While broader health system strengthening is necessary, prioritizing adolescent health and female education within PHC systems appears to offer the most promising pathway for reducing maternal mortality in the highest-burden settings.
Recommendation
Based on our findings, we recommend the following evidence- based strategies: Governments should develop adolescent- responsive services within PHC systems, including comprehensive sexual education, youth-friendly health services, and accessible family planning [17,18]. They should integrate adolescent sexual and reproductive health into PHC packages. The strong correlation shown in Fig. 1 suggests that reducing adolescent birth rates by 50% could potentially reduce maternal mortality by 37-40% in high-burden countries. Ministries of education and health should collaborate to ensure girls' access to secondary education, recognizing education as a critical social determinant of maternal health [14,25]. They should accelerate multi-sectoral investments in female education. The "L-shape" pattern in Fig. 3 indicates that increasing female secondary education from 15% to 40% could yield the most dramatic reductions in maternal mortality.
International donors and regional bodies should create specialized PHC packages for Sub-Saharan Africa that simultaneously address service delivery gaps and social determinants [8,16]. They should develop Sub-Saharan Africa specific PHC strengthening initiatives. The regional analysis in Fig. 2 demonstrates that this region requires intensified, multi-pronged approaches tailored to its unique challenges. Countries should adopt PHC performance measurement frameworks, such as those developed by PHCPI, to track progress in strengthening the specific PHC dimensions most critical to maternal survival [6,7]. They should enhance PHC performance measurement and accountability. The weak association in Fig. 4 suggests that political empowerment should be coupled with robust accountability mechanisms for health outcomes.
Governments and development partners should implement equitable financing strategies that reduce financial barriers to maternal health services, particularly for adolescents and underserved populations [24,26]. They should prioritize pro-poor financing mechanisms. The extreme disparities in Table 4 highlight the need for targeted financial protection for the most vulnerable. Governments should strengthen community-based PHC delivery by implementing task-shifting strategies and community health worker programs to extend PHC reach in remote and underserved areas, focusing on maternal health education, antenatal care, and skilled birth attendance promotion [27].
Future research should conduct implementation research on effective PHC models identifying the most effective implementation strategies for strengthening priority PHC dimensions in various contexts, with particular attention to fragile and conflict-affected settings where maternal mortality burdens are highest [28,29]. Governments should establish real-time maternal health surveillance systems. They should develop and strengthen health information systems to track maternal mortality and PHC service coverage in real-time, enabling rapid response to emerging challenges and more effective resource allocation [13,30]. These recommendations, grounded in the empirical patterns revealed through our analysis, provide a roadmap for accelerating progress toward the SDG maternal health targets. By focusing on the PHC dimensions most strongly associated with maternal survival— particularly adolescent health services and female education— countries can achieve more efficient and equitable reductions in maternal mortality.
Consent for Publication
Not applicable.
Funding
This research received no external funding.
Credit Authorship Contribution Statement
Rachael Gakii Murithi: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing - original draft.
Beiran Qian: Data curation, Investigation, Visualization, Writing - review & editing.
Kun Tang: Supervision, Writing - review & editing.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments
Not applicable.
References
- World Health Organization. (2019). Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division.
- World Health Organization. (1978). Regional Office forE. Declaration of Alma-Ata. Copenhagen: World Health Organization. Regional Office for Europe; 1978 1978. Contract No.: WHO/EURO, 3938-43697.
- Sharrow, D., Hug, L., You, D., Alkema, L., Black, R., Cousens, S., ... & Walker, N. (2022). Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. The Lancet Global Health, 10(2), e195-e206.
- World Health Organization. Declaration of astana. WorldHealth Organization. 2018.
- Kruk, M. E., Gage, A. D., Arsenault, C., Jordan, K., Leslie,H. H., Roder-DeWan, S., ... & Pate, M. (2018). High-quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet global health, 6(11), e1196-e1252.
- Veillard, J., Cowling, K., Bitton, A., Ratcliffe, H., Kimball, M., Barkley, S., ... & Wang, H. (2017). Better measurement for performance improvement in low-and middle-income countries: the primary health care performance initiative (PHCPI) experience of conceptual framework development and indicator selection. The Milbank Quarterly, 95(4), 836-883.
- Primary Health Care Performance Initiative. About PHCPI | PHCPI. 2022.
- Memirie, S. T., Verguet, S., Norheim, O. F., Levin, C., & Johansson, K. A. (2016). Inequalities in utilization of maternal and child health services in Ethiopia: the role of primary health care. BMC health services research, 16(1), 51.
- Russo, L. X., Scott, A., Sivey, P., & Dias, J. (2019). Primary care physicians and infant mortality: evidence from Brazil. PLoS One, 14(5), e0217614.
- Shi, L., Macinko, J., Starfield, B., Xu, J., Regan, J., Politzer, R., & Wulu, J. (2004). Primary care, infant mortality, and low birth weight in the states of the USA. Journal of Epidemiology & Community Health, 58(5), 374-380.
- De Bernis, L., Sherratt, D. R., AbouZahr, C., & Van Lerberghe,W. (2003). Skilled attendants for pregnancy, childbirth and postnatal care. British medical bulletin, 67(1), 39-57.
- Graham, W. J., Bell, J. S., & Bullough, C. H. (2001). Can skilled attendance at delivery reduce maternal mortality in developing countries?. Safe motherhood strategies: a review of the evidence.
- Campbell, O. M., Calvert, C., Testa, A., Strehlow, M., Benova, L., Keyes, E., ... & Bailey, P. (2016). The scale, scope, coverage, and capability of childbirth care. The Lancet, 388(10056), 2193-2208.
- Schnell-Anzola, B., Rowe, M. L., & LeVine, R. A. (2005). Literacy as a pathway between schooling and health-related communication skills: a study of Venezuelan mothers. International Journal of Educational Development, 25(1), 19-37.
- Luo, Z., Wilkins, R., & Kramer, M. S. (2006). Effect of neighborhood income and maternal education on birth outcomes: a population-based study. NEONATAL INTENSIVE CARE, 19(6), 48.
- Hanson, K., Brikci, N., Erlangga, D., Alebachew, A., De Allegri, M., Balabanova, D., ... & Wurie, H. (2022). The Lancet Global Health Commission on financing primary health care: putting people at the centre. The Lancet Global Health, 10(5), e715-e772.
- Besnier, E., Thomson, K., Stonkute, D., Mohammad, T., Akhter, N., Todd, A., ... & Bambra, C. (2021). Which public health interventions are effective in reducing morbidity, mortality and health inequalities from infectious diseases amongst children in low-and middle-income countries (LMICs): an umbrella review. PLoS One, 16(6), e0251905.
- Okonofua, F. E., Ntoimo, L. F., Adejumo, O. A., Imongan, W., Ogu, R. N., & Anjorin, S. O. (2022). Assessment of interventions in primary health care for improved maternal, new-born and child health in Sub-Saharan Africa: a systematic review. Sage Open, 12(4), 21582440221134222.
- Kruk, M. E., Gage, A. D., Arsenault, C., Jordan, K., Leslie,H. H., Roder-DeWan, S., ... & Pate, M. (2018). High-quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet global health, 6(11), e1196-e1252.
- Browne, A. J., Varcoe, C. M., Wong, S. T., Smye, V. L., Lavoie, J., Littlejohn, D., ... & Lennox, S. (2012). Closing the health equity gap: evidence-based strategies for primary health care organizations. International journal for equity in health, 11(1), 59.
- The World Bank. World Bank Gender Data Portal. The World Bank Group. Last modified 2025.
- Bitton, A., Ratcliffe, H. L., Veillard, J. H., Kress, D. H.,Barkley, S., Kimball, M., ... & Hirschhorn, L. R. (2017). Primary health care as a foundation for strengthening health systems in low-and middle-income countries. Journal of general internal medicine, 32(5), 566-571.
- Obeagu, E. I., & Obeagu, G. U. (2024). An update on factors affecting umbilical cord care among mothers: A review. Medicine, 103(28), e38945.
- Limwattananon, S., Tangcharoensathien, V., & Prakongsai,P. (2010). Equity in maternal and child health in Thailand.Bulletin of the World Health Organization, 88, 420-427.
- Lengkong, J. S., Rotty, V. N., Teol, M., Rawis, J. A., & Kalalo,D. K. (2023). Development of the Maternal and Child Health Education Model in North Sulawesi Province. International Journal of Multicultural and Multireligious Understanding, 10(5), 359-375.
- Eschliman, B. H., Pham, H. H., Navathe, A. S., Dale, K. M., & Harris, J. (2023). The role of payment and financing in achieving health equity. Health Services Research, 58, 311- 317.
- Herrera, J. A. (2013). Primary care and maternal and infant mortality in Latin American countries. Atencion Primaria, 45(5), 244-248.
- Althubaiti, A. (2023). Sample size determination: A practical guide for health researchers. Journal of general and family medicine, 24(2), 72-78.
- Costa-Nobre, D. T., Kawakami, M. D., Areco, K. C. N.,Sanudo, A., Balda, R. C. X., Marinonio, A. S. S., ... & Kiffer,C. R. V. (2021). Clusters of cause specific neonatal mortality and its association with per capita gross domestic product: A structured spatial analytical approach. Plos one, 16(8), e0255882.
- Sharrow, D., Hug, L., You, D., Alkema, L., Black, R., Cousens, S., ... & Walker, N. (2022). Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. The Lancet Global Health, 10(2), e195-e206.