
International Journal of Endocrinology Research and Reviews(IJERR)
ISSN: 2993-656X | DOI: 10.33140/IJERR

Research Article - (2024) Volume 4, Issue 1
Adherence to Lifestyle Modifications and Correlates Among Hypertensive Patients Attending Chronic Follow-Up at Asella Referral and Teaching Hospital, Southeast Ethiopia
Received Date: Jan 08, 2024 / Accepted Date: Feb 06, 2024 / Published Date: Mar 15, 2024
Copyright: ©©2024 Kedir Negesso Tukeni, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Dekema, R. J., Tukeni, K. N. (2024). Adherence to Lifestyle Modifications and Correlates Among Hypertensive Patients Attending Chronic Follow-Up at Asella Referral and Teaching Hospital, Southeast Ethiopia. Int J Endo Res & Rev, 4(1), 01-07.
Abstract
Background Around the world, hypertension is a serious health issue. Hypertension left unchecked might cause difficulties. In addi- tion to pharmacological therapy, lifestyle changes must still be adhered to as an essential aspect of care. The purpose of this study was to evaluate factors that influence how well hypertension patients at Asella Referral Hospital in South East Ethiopia adhere to lifestyle changes.
Methodology Between September 1 and January 30 of 2021, the Asella Referral Hospital hosted this hospital-based cross-sectional study. All individuals with a diagnosis of hypertension who were being followed up on during the trial period were included. Data were gathered through the use of structured questionnaires and entered into Epi-data for analysis. The associations between the variables were investigated using chi-square tests and logistic regression models
Results There were 289 hypertensive patients, 48.8% of whom were men and 51.6% of whom were in the 40–59 age range. Over half (56.7%) of the participants went to primary school, and as a result, they can read and write. Nearly 40% of research participants work for themselves in the private sector, and more than 60% said their families support them in managing their hypertension. The majority of research participants (77.9%) reported poor lifestyle change adherence. Low monthly income (AOR=2.88; 95%CI=1.08-7.69), comorbidity, inadequate hypertension knowledge (AOR=1.98; 95% CI=1.06-3.69), and longer duration of hypertension (AOR=3.35; 95% CI =1.19-9.47), all of which were associat- ed with poor adherence to lifestyle change.
Conclusion In this study, there was poor adherence to lifestyle adjustment among hypertension patients. Lack of information, low family income, a longer time frame, and the existence of comorbidities were the main predictors of poor adherence to lifestyle changes. This underlines the significance of public health awareness, better health insurance coverage, and the treatment of co-morbidities may enhance adherence to lifestyle changes, which lower morbidity and mortality while enhancing survival and quality of life.
Keywords
Hypertension, Adherence, Lifestyle Modification, Asella Referral Hospital, Ethiopia
Introduction
Non-Communicable Diseases (NCDs) are the leading cause of morbidity and mortality in many countries and have reached epidemic proportions globally [1]. Hypertension is one of the most common NCDs and growing global health problems in the world. Hypertension can be defined as systolic blood pressure (SBP) greater than or equal to 140 mm Hg and diastolic blood pressure (DBP) greater than or equal to 90 mm Hg over a sustained period, based on the average of two or more blood pressure measurements taken in two or more contacts with the health care provider after an initial screening [2].
In emerging nations, hypertension is increasingly contributing to morbidity and mortality. Additionally, it adds to the burden of premature mortality, disability, kidney failure, heart disease, and stroke [3, 4]. Worldwide, hypertension is responsible for 51% of fatalities from stroke and 45% of deaths from heart disease. Approximately 46% of persons in Africa who are 25 years of age and older have hypertension, compared to 35 to 40% globally.
The frequency of hypertension is rising in Sub-Saharan African nations, where 75 million adults are affected. In the next 10 to 15 years, it is predicted that the prevalence would increase to 125.5 million.4 Evidence at this time shows that the rise in modifiable risk factors is contributing to an increase in the incidence of hypertension and its complications [5]. Controlling hypertension and its complications has mostly been hampered by poor adherence to advised lifestyle changes5. Scientific research has repeatedly shown that a risk factor for hypertension increases the risk of stroke, contributes to excess caloric intake, and can lessen the effectiveness of antihypertensive drugs [6].
The most crucial first step in treating a hypertensive patient is lifestyle change, which includes reducing sodium intake, exercising regularly, quitting smoking, consuming alcohol in moderation, and following the doctor's instructions for the DASH diet [7]. Poor adherence or noncompliance can lower quality of life and raise medical care costs [8]. The general mortality rates may be significantly impacted by these lifestyle changes [9]. According to the evidence, the risk factors for developing hypertension, such as smoking, obesity, drinking alcohol harmfully, and not exercising, are on the rise. The prevalence of hypertension in Ethiopia ranges from 27.8% to 31.5% [10].
Whether or not they are taking hypertension medication, all hypertensive patients should exercise lifestyle adjustment, according to The Seventh Report of the Joint National Committee. Evidence from the prior studies suggests that combining lifestyle changes with medical therapy to treat hypertension is a very effective strategy . Nine worldwide NCD targets were set by the WHO worldwide Action Plan for the Prevention and Control of NCDs to lower the prevalence of high blood pressure by 25%. Stroke, myocardial infarction, cardiac failure, and renal failure are just a few of the catastrophic effects of hypertension [5, 7, 11-15].
Our nation, Ethiopia, has incorporated non-communicable disease in the national nutrition program and sustainable development goals to prevent the consequences of hypertension described above. However, the prevalence of hypertension and associated complications are not under control due to a lack of food-based guidelines in the nation and low adherence to lifestyle practices among those who have been classified as hypertensive [16].
The incidence of hypertension and the impact of sociodemographic factors on adherence were the main points of emphasis in earlier investigations [10, 17]. Despite the fact that Socio-demographic factors have a significant influence on how patients manage their condition, a variety of independent factors that may affect patients' adherence to lifestyle change have received little research. Few research is carried out in Ethiopia, despite the fact that the problem of poor adherence to lifestyle change calls for intense devotion and considerable attention. In the current study area, there has also been no research on what factors contribute to poor adherence. Therefore, the purpose of this study was to evaluate how well hypertension patients who attended chronic follow-up clinics at Asella hospital adhered to lifestyle modification and the characteristics that were associated with it.
Material and methods
Study Design and Setting
From September 1 to November 30, 2021, a quantitative prospective observational hospital-based study was carried out at the Asella Referral and Teaching Hospital in Ethiopia. The Asella Referral Hospital is a tertiary teaching hospital with a catchment area of more than 4 to 5 million people. It is situated in Asella Town, Arsi Zone in Oromia region, Ethiopia. The teaching hospital has more than 320 beds, 1500 medical professionals, 10,000 emergency cases, and more than 4000 deliveries each year. It also serves about 100,000 outpatients. The hospital offers a variety of inpatient services, including electrocardiogram and echocardiography for patients with hypertension, as well as other important facilities, including diabetes care and follow¬up, higher imaging services, including computed tomography. It also offers outpatient follow-up clinics, emergency care services, particularly for spectrums of acute coronary syndromes.
Inclusion and Exclusion Criteria
During the study period, all patients >18 years old with hypertension who were taking medication and receiving follow¬up care at the Asella Referral and Teaching Hospital, were willing to participate in the study, and provided written informed consent. Patients with a diagnosis of hypertension who declined to take part in the trial or those whose follow-up very recently began were not included.
Sample Size Determination
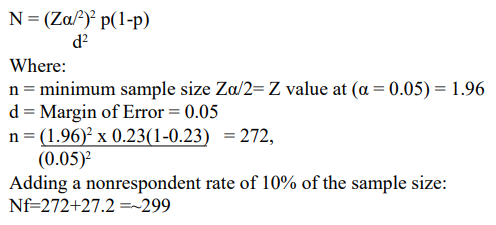
The single population proportion formula was used to calculate the sample size while taking into account the following hypotheses: 95% confidence interval (CI), 23% of hypertension patients adhering to lifestyle changes from the Addis Abeba study18, with a 5% margin of error, and computed as follows:
Data Collection
The Socio-demographic characteristics (age, sex, chart number, marital status, level of education, monthly income, and area of residence) and clinical profiles of the patients with hypertension, with a focus on the medication and lifestyle adherence, were collected using a structured data collection format that was tested for consistency prior to data collection. The patient records were gathered and examined for additional information about prior patient treatment, the type and dosage of medications the patients took, prior admission history, and potential causes and management discussed in the current presentation. The risk of infection transmission from patients to the data collectors and vice versa was decreased by the use of personal protective equipment by the data collectors, such as face masks and alcohol-based hand sanitizers.
Data Analysis
Epidata management version 3.1 was used to examine the data before it was transferred to SPSS version 26. The study participants' demographic details underwent a descriptive analysis. Categorical data are displayed in graphs and pie charts and were analyzed using frequencies (n) and percentages (%). The mean (SD) for normally distributed data or the median (IQR) for skewed data were used to examine continuous data. Bivariate analysis included the use of chi-square, Fisher's exact, and student data, while multivariate analysis included the use of binary logistic analysis. When the cell frequency was less than five (n5), Fischer's exact test was applied, and when the cell frequency was greater than five (n>5), the chi-square test was applied. At P 0.05, the significance level was established. The direction of the link between the independent and dependent variables was demonstrated using the odds ratio.
Study Limitation
It was unable to determine the causal association between the research variables because this was a cross-sectional study. Additionally, it only covered individuals who had been admitted to the hospital. Along with the small sample size, it is challenging to pinpoint criteria that apply to admitted cases as opposed to non-admitted patients who may be referred to another facility or even pass away while receiving follow-up care. Additionally, the fact that this result came from a single institution has an impact on generalizability
Results
Socio-Demographic Characteristics
During the study period, 289 patients with hypertension who were receiving follow-up care at Asella Referral and Teaching Hospital were interviewed and included in the study, with a 96.65% response rate. The majority of research participants were female (51.2%, with a male to female ratio of 1:1.05), and the average age was 56 12 years. The majority of patients (56.7%) had completed their primary school and were from an urban area (74.4%). The average yearly income of survey participants was around 430 USD for 90.7% of them. Ninety-seven percent of the patients were married and all of them were housed with their families. Even though more than half of the study participants (61.9%) had family support, a sizable portion (38.1%) did not stick to the regimen in a sufficient manner Table 1.
|
Variables |
Category |
Frequency(n=289) |
Percent (100%) |
|
Residency |
Urban |
215 |
74.4 |
|
Rural |
74 |
25.6 |
|
|
Sex |
Male |
141 |
48.8 |
|
Female |
148 |
51.2 |
|
|
Age |
21-39 |
16 |
5.5 |
|
40-59 |
149 |
51.6 |
|
|
>60 |
124 |
42.9 |
|
|
Marital status |
Single |
2 |
.7 |
|
Married |
283 |
97.9 |
|
|
Divorced |
2 |
.7 |
|
|
Widowed |
2 |
.7 |
|
|
Educational status |
can't read and write |
112 |
38.8 |
|
Primary |
164 |
56.7 |
|
|
secondary and above |
13 |
4.5 |
|
|
Occupational status |
government-employed |
7 |
2.4 |
|
private worker |
125 |
43.3 |
|
|
Housewife |
69 |
23.9 |
|
|
Retired |
34 |
11.8 |
|
|
Farmer |
54 |
18.7 |
|
|
Monthly Income (17) |
<1000 |
21 |
7.3 |
|
1000-1999 |
6 |
2.1 |
|
|
>2000 |
262 |
90.7 |
|
|
Family Support for adherence |
Yes |
179 |
61.9 |
|
No |
110 |
38.1 |
Table 1: Socio-demographic characteristics of respondents at Asella referral hospital chronic follow-up unit (n=289), 2021
Medical Characteristics, Lifestyle Modification Adherence and Correlates of the Study Participants
140 (48.4%) of the 289 hypertensive patients had been that way for more than five years, and 90% of the study participants said they knew enough about lifestyle changes to control their hypertension. Cardiovascular disorders and diabetes mellitus were the two comorbidities that were most prevalent, affecting more research participants Table 2.
|
Variable |
Category |
Frequency |
Percent |
|
Duration since diagnosed |
<2 years |
65 |
22.5 |
|
2-5 years |
84 |
29.1 |
|
|
>5 years |
140 |
48.4 |
|
|
Comorbidity |
No |
174 |
60.2 |
|
Yes |
115 |
39.8 |
|
|
Types of Comorbidities (n=115) |
Diabetes mellitus |
59 |
20.4 |
|
CKD |
6 |
2.1 |
|
|
Cardiovascular disease |
51 |
17.6 |
|
|
Information about healthy lifestyle |
Yes |
255 |
88.2 |
|
No |
34 |
11.8 |
|
|
Source of information |
medical staff |
247 |
85.5 |
|
Media |
36 |
12.5 |
|
|
family and friend |
4 |
1.4 |
|
|
Other |
2 |
.7 |
|
|
Care provider communication |
Poor |
68 |
23.5 |
|
Good |
221 |
76.5 |
|
|
Self- efficacy |
poor self-efficacy |
134 |
46.4 |
|
good self-efficacy |
155 |
53.6 |
Table 2: Medical characteristics of respondents at Asella referral hospital chronic follow-up unit (n=289), 2021
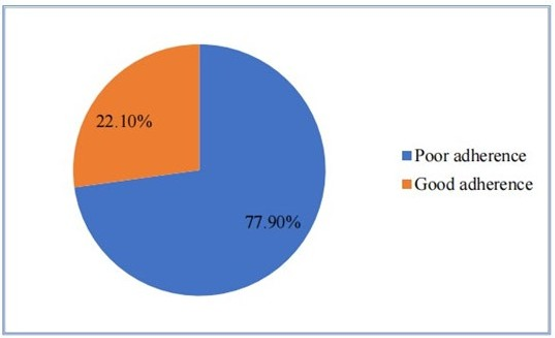
Figure 1: Level of adherence among hypertensive patients on follow up at Asella Referral and Teaching Hospital, 2021

Figure 2: Adherence patterns among hypertensive patients on follow up at Asella Referral and Teaching Hospital, 2021
Insufficient adherence to lifestyle changes to control their hyper-tension affected more than two-thirds (77.9%) of the study participants Figures 1 and 2. Poor adherence to lifestyle modification was found to be negatively correlated with level of knowledge about hypertension (AOR= 1.98; 95% CI=1.06-3.69), presence of comorbidity (AOR=1.72; 95% CI=1.0-3.23), time since the diagnosis of hypertension (AOR=3.35; 95% CI =1.19-9.47), and income (AOR=2.88; 95% CI=1.08-7.69) Table 3.
|
Variables |
Adherence to lifestyle modification |
COR (95%CI) |
AOR (95%CI) |
p-value |
|
|
Good |
Poor |
||||
|
Knowledge about hypertension |
|
|
|
|
|
|
Good |
43 |
109 |
1 |
1 |
0.032* |
|
poor |
21 |
116 |
2.18[1.22-3.91] |
1.98[1.06-3.69] |
|
|
Comorbidity |
|
|
|
|
|
|
No |
43 |
131 |
1 |
1 |
|
|
Yes |
21 |
94 |
1.47[1.00-2.64] |
1.72 [1.00-3.23] |
0.01* |
|
Residence |
|
|
|
|
|
|
Urban |
44 |
171 |
1 |
1 |
|
|
|
|
|
|
|
|
|
Rural |
20 |
54 |
0.69[0.37-1.28] |
0.54[0.28-1.03] |
0.06 |
|
Duration since diagnosed |
|
|
|
|
|
|
<2 years |
8 |
57 |
1.36[0.72-2.59] |
1.24[0.63-2.42] |
.533 |
|
2-5years |
18 |
66 |
2.65[1.16-6.01] |
3.35[1.19-9.47] |
.023* |
|
≥5years |
38 |
102 |
1 |
1 |
|
|
Income |
|
|
|
|
|
|
<1000 |
9 |
12 |
0.33[0.13-.83] |
2.88[1.08-7.69] |
.035* |
|
1000-1999 |
3 |
3 |
0.25[0.05-1.26] |
0.24[0.03-1.95] |
0.181 |
|
>2000 |
52 |
210 |
1 |
1 |
|
Note: * P-value<0.05 AOR: adjusted odds ratio, CI: confidence interval, COR: crude odds ratio
Table 3: Factors associated with Adherence to lifestyle modification among hypertensive patients attending chronic follow-up clinic of Asella referral hospital 2021.
Discussion
Male to female participants in the study made up 51.2%, with the majority of participants aged 40 to 59. According to the survey, only 77.9% of individuals adhered to their new lifestyles. This result was less than that of studies conducted in Serbia, Ghana, Durame, and Addis Abeba, which found that the rates of adherence to lifestyle change were, respectively, 35%, 72%, 27%, and 23% [14, 17-19].
There are a number of factors that contribute to poor adherence, and this study found that knowledge of hypertension (AOR= 1.98; 95% CI= 1.06-3.69) was one of these factors. This result was consistent with a study that demonstrated the importance of information for hypertension patients in order for them to implement the proper lifestyle modification strategies18. Another study done elsewhere revealed that a significant number of hypertension patients were ignorant of their condition and needed lifestyle changes.
As 39.8% of participants had comorbidity, this study also found that poor adherence was related with comorbidity (AOR=1.72; 95% CI=1.0-3.23), which is consistent with findings from cross-sectional studies conducted in Durame and Saudi Arabia12. Many hypertensive Africans are not aware of their illness, and their hypertension and concomitant disorders are either not treated or are inadequately managed, which puts them at the highest risk for consequences such heart disease, stroke, and renal and cardiac disease. Of the people that have hypertension, almost 50% are unaware that they have elevated blood pressure in Africa [20, 21].
Another factor that contributed to poor adherence to lifestyle change was the length of hypertension (AOR=3.35;95% CI =1.19-9.47). This was also consistent with the results of a study done in Ghana, where it was discovered that the longer time after hypertension was detected was associated with poor commitment to lifestyle adjustment19. Additionally, the study participants' adherence to lifestyle change was significantly impacted by their income level (AOR=2.88; 95%CI=1.08-7.69). This is comparable to other research that showed low socioeconomic position and low money were barriers to maintaining a lifestyle change [17-19].
Conclusion
In this study, there was poor adherence to lifestyle adjustment among hypertension patients. Lack of information, low family income, a longer time frame, and the existence of comorbidities were the main predictors of poor adherence to lifestyle changes. This underlines the significance of public health awareness, better health insurance coverage, and the treatment of co¬morbidities may enhance adherence to lifestyle changes, which lower morbidity and mortality while enhancing survival and quality of life.
Data sharing Statement
All data are available within the article.
Ethical Approval
The Institutional Review Board (IRB) of the Institute of Health, Arsi University, granted ethical approval. It was possible to secure an official letter of support from the relevant administration. The goal of the study was explained to each participant and their relevant stakeholders, and each participant provided their signed informed permission. For individuals who couldn't read or write, we used an impartial witness throughout the full informed consent procedure and data collecting phase. The Helsinki Declaration was followed when conducting the study. Instead, then using personal identification, unique codes were used to maintain the confidentiality of the participants' information.
Acknowledgment
We appreciate the staff at the Asella Referral and Teaching Hospital as well as the other medical experts who assisted with the study in the Chronic Follow-Up Clinic.
Author Contributions
The main text was written by RJD and KNT. The manuscript was revised by RJD and KNT. RJD and KNT carried out the analysis. The manuscript was examined by both writers. Additionally, they decided on the journal to which the paper was submitted, gave their final approval of the version that would be published, and pledged to take responsibility for every part of the effort.
Funding
No specific grants for this research were given by any funding organizations in the public, private, or nonprofit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
- WHO. (2017). Noncommunicable diseases progress monitor 2017. World Health Organization.
- Forouzanfar, M. H., Liu, P., Roth, G. A., Ng, M., Biryukov, S., Marczak, L., ... & Murray, C. J. (2017). Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990-2015. Jama, 317(2), 165-182.
- Warren-Findlow, J., Seymour, R. B., & Brunner Huber,L. R. (2012). The association between self-efficacy and hypertension self-care activities among African American adults. Journal of community health, 37, 15-24.
- World Health Organization. (2016). Action plan for the prevention and control of noncommunicable diseases in the WHO European Region (No. WHO/EURO: 2016-2582-42338-58618). World Health Organization. Regional Office for Europe.
- Chobanian, A. V., Bakris, G. L., Black, H. R., Cushman, W. C., Green, L. A., Izzo Jr, J. L., ... & National High Blood Pressure Education Program Coordinating Committee. (2003). Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. hypertension, 42(6), 1206-1252.
- Warren-Findlow, J., & Seymour, R. B. (2011). Prevalence rates of hypertension self-care activities among African Americans. Journal of the National Medical Association, 103(6), 503-512.
- Al-Wehedy, A., Abd Elhameed, S. H., & Abd El-Hameed,D. (2014). Effect of lifestyle intervention program on controlling hypertension among older adults. Journal of Education and Practice, 5(5), 61-71.
- Kamran, A., Azadbakht, L., Sharifirad, G., Mahaki, B., & Mohebi, S. (2015). The relationship between blood pressure and the structures of Pender's health promotion model in rural hypertensive patients. Journal of education and health promotion, 4.
- Lifestyle modifications for hypertension management | Egyptian Journal of Hospital Medicine [The]. 2018; 70(12): 2152-2156 | IMEMR. Accessed September 29, 2023. https://pesquisa.bvsalud.org/portal/resource/pt/emr-192781
- Kalssa, A., Ayele, G., Tamiso, A., & Girum, T. (2016). Prevalence and associated factors of Hypertension among civil servants working in Arba Minch Town, South Ethiopia. International Journal of Public Health Science (IJPHS), 5(4), 375-383.
- Baker-Smith, C. M., Flinn, S. K., Flynn, J. T., Kaelber, D.C., Blowey, D., Carroll, A. E., ... & Urbina, E. M. (2018). Diagnosis, evaluation, and management of high blood pressure in children and adolescents. Pediatrics, 142(3).
- Elbur, A. I. (2015). Level of adherence to lifestyle changes and medications among male hypertensive patients in two hospitals in Taif; Kingdom of Saudi Arabia. Int J Pharm Pharm Sci, 7(4), 168-172.
- Nepal, P., & Dhungana, B. (2015). Lifestyle modification after diagnosis of hypertension in patients visiting Lumbini Medical College Teaching Hospital. Journal of Lumbini Medical College, 3(1), 12-15.
- Andjelkovic, M., Mitrovic, M., Nikolic, I., Jovanovic, D. B., Zelen, I., Zaric, M., ... & Jankovic, S. (2017). Older hypertensive patients’ adherence to healthy lifestyle behaviors. Serbian Journal of Experimental and Clinical Research, 19(1), 51-56.
- Bruno, C. M., Amaradio, M. D., Pricoco, G., Marino, E., & Bruno, F. (2018). Lifestyle and hypertension: An evidence-based review. J Hypertens Manag, 4(1), 1-10.
- Geremew, G., Ambaw, F., Bogale, E. K., & Yigzaw, Z. A. (2023). Adherence to Lifestyle Modification Practices and Its Associated Factors Among Hypertensive Patients in Bahir Dar City Hospitals, North West Ethiopia. Integrated Blood Pressure Control, 111-122.
- Buda, E. S., Hanfore, L. K., Fite, R. O., & Buda, A. S. (2017). Lifestyle modification practice and associated factors among diagnosed hypertensive patients in selected hospitals, South Ethiopia. Clinical hypertension, 23(1), 1-9.
- Tibebu, A., Mengistu, D., & Negesa, L. (2017). Adherence to recommended lifestyle modifications and factors associated for hypertensive patients attending chronic follow-up units of selected public hospitals in Addis Ababa, Ethiopia. Patient preference and adherence, 323-330.
- Obirikorang, Y., Obirikorang, C., Acheampong, E., Anto,E. O., Amoah, B., Fosu, E., ... & Asiwu, R. Y. (2018).Adherence to lifestyle modification among hypertensive clients: a descriptive cross-sectional study. Open Access Library Journal, 5(2), 1-13
- Dzudie, A., Rayner, B., Ojji, D., Schutte, A. E., Twagirumukiza, M., Damasceno, A., ... & Awad, M. (2017). PASCAR Roadmap on Hypertension. CARDIOVASCULAR JOURNAL OF AFRICA, 28(4), 261-272.
- Guwatudde, D., Nankya-Mutyoba, J., Kalyesubula, R., Laurence, C., Adebamowo, C., Ajayi, I., ... & Dalal, S. (2015). The burden of hypertension in sub-Saharan Africa: a four-country cross sectional study. BMC public health, 15, 1-8.