
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2019) Volume 1, Issue 1
Acute Kidney Injury in Children: Etiologies and Results
Received Date: Feb 18, 2019 / Accepted Date: Feb 26, 2019 / Published Date: Mar 04, 2019
Copyright: ©A Seba, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Acute kidney Injury (AKI) is characterized by a reversible increase in the blood concentration of creatinine and nitrogenous waste products and by the inability of the kidney to regulate fluid and electrolyte homeostasis appropriately [1]. There are many causes of AKI.
Introduction
Acute kidney Injury (AKI) is characterized by a reversible increase in the blood concentration of creatinine and nitrogenous waste products and by the inability of the kidney to regulate fluid and electrolyte homeostasis appropriately [1]. There are many causes of AKI.
Some causes of AKI, such as rapidly progressive glomerulonephritis (RPGN), may present as AKI but rapidly evolve into chronic kidney disease (CKD). Several renal diseases, such as the hemolytic–uremic syndrome (HUS), Henoch–Schönlein purpura, and obstructive uropathy with associated renal dysplasia, may present as AKI with improvement of renal function to normal or near-normal levels, but the child’s renal function may slowly deteriorate, leading to CKD several months to years later.
Methods
Type of study: Our study is retrospective. It was conducted in the Department of Nephrology of the University Hospital Center (UHC) of Tizi Ouzou, between 2015 and 2018.
The patients were selected from the hospitalization register. We included all children with acute renal injury during this time period.
Evidence Collected: Data was collected from patients’ medical records. We found the following: - Age, sex, etiological diagnosis, evolution.
Results
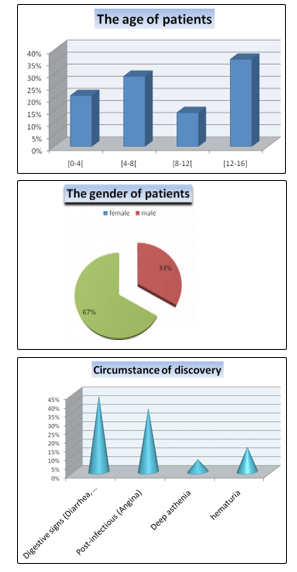
Over the four years, 26 patients (34% male) with a median age of 7 years (range 40 days to 15 years) were managed. The most affected age group in our study is [12-16] with a frequency of 36%.
The circumstances of discovery in the majority of our patients being revealed by digestive signs (diarrhea, vomiting) and that related to the etiology of AKI (HUS post diarrhea).
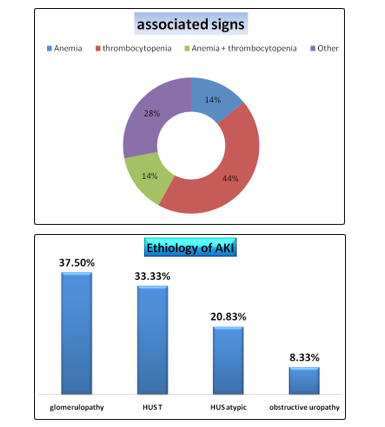
In our study, 44% of the patients have thrombocytopenia associated with AKI; and this is due to the origin of this syndrome (Atypical HUS).
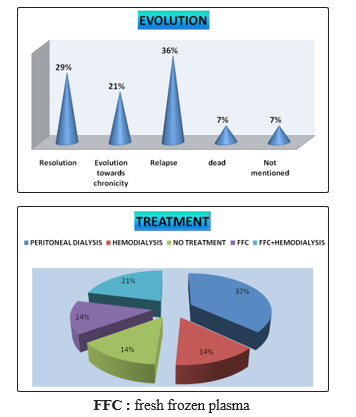
The etiology of AKI is: Nephropathy glomerular in 37% HUS in 54% and obstructive nephropathy in 9%. Patients survived in 92 % of the cases and 58% of them had a normal renal function. We had 7% of death.
Peritoneal dialysis is the most commonly used emergency treatment for AKI in children at a frequency of 37%. Also Hemodialysis is more used
Discussion
The prevalence of AKI is variously appreciated in the literature. Most of the data come from intensive care units, post-surgery resuscitation, neonatology or nephrology where the type of recruitment of children is different from one service to another [2].
The average age of the children in our work was 7 years. In 2001, in a pediatric ward in Alabama (USA) Bunchmann et al. reported an average age of 6.16 years. Most authors agree that the etiologies of AKI in children vary by age.
Despite variations, two causes dominate, AKI secondary to renal hypoperfusion and Hemolytic Uremic Syndrome (HUS) [1-4]. The first cause occurs at any age, while HUS, in typical form, is unique to infants and young children under three years of age, in our experience.
Five patients (36%) were feverish at admission. This testifies to the responsibility of infections in the genesis of nephropathies.
The severity of the renal involvement seems to affect the renal functional prognosis. Indeed, elevated serum creatinine and blood urea are predictive of renal failure. The kidney is the only emunctory potassium and the risk of hyperkalemia exists as soon as an AKI sets up. Any serum potassium greater than 6mmol / l is at risk for severe heart rythm disorders. Anemia was found in two patients (14%).
Etiologically, the most common cause in our study was atypical HUS with a frequency of 58%. In neonates, hypoperfusion was the leading cause of AKI. Post infectious glomerulonephritis was present in 36% of cases in our study. Its frequency is appreciated in the USA with 12.6% cases i. The acute glomerulonephritis in a tropical environment is post-streptococcal and is often associated with an AKI. Recovery is usually complete and does not require biopsy. However, biopsy may be indicated in cases of rapidly progressive glomerulonephritis.
In other studies, organic AKI of toxic origin is described. This nephrotoxicity is observed in oncology in children treated with Cisplatin or Methotrexate. Causes of post-renal AKI in children are uncommon.
Therapeutically, peritoneal dialysis practiced in the majority of the cases, hemodialysis was prescribed in 14% of our patients [5]. Currently, because of the effectiveness of extra-renal cleansing techniques, mortality is most often linked to the etiological context and not to the consequences of AKI. The treatment of glomerular AKI depends, of causes of their etiologies. They sometimes use corticosteroids, immunosuppressants, or plasma exchanges
On the evolutionary level, 04 patients (29%) had evolved favorably, with a complete recovery of renal function. An AKI poorly supported, or the installation of a bilateral cortical necrosis immediately evolve the patient to the chronicity noted in 03% of our patients. In our study, we noted death in 7% of patients.
Conclusion
The occurrence of Acute kidney Injury (AKI) in child is a fairly common situation that requires a diagnostic approach: recognize etiology (functional, obstructive or organic AKI) and clinical and biological disturbances to implement quickly route the adapted therapy. It is also important to emphasize the prevention of kidney failure in risk situations. The long-term prognosis of AKI in child depends on their etiology.
References
- Sharon Phillips Andreol (2009) Acute kidney injury in children. Pediatr Nephrol 24: 253-263.
- Kadar Ismail Hassan, Jama Hodan M, Chunfu Li . Cureus (2017) A Retrospective Study of Acute Renal Failure in Children: Its Incidence, Etiology, Complications and Prognosis 9: e1274.
- Prasad Devarajan (2014) Pediatric Acute Kidney Injury: Different From Acute Renal Failure But How and Why, CurrPediatr Rep 1: 34-40.
- Alaleh Gheissari, Pardis Mehrasa, Alireza Merrikhi, Yahya Madihi (2012) Acute kidney injury: A pediatric experience over 10 years at a tertiary care center, J Nephropathology 1: 101-108.
- Vladimirs Strazdins, Alan R. Watson, Ben Harvey (2004) Renal replacement therapy for acute renal failure in children: European Guidelines , Pediatr Nephrol 19: 199-207.