
COVID Research: Open Access(CROA)
ISSN: 2995-7826 | DOI: 10.33140/CROA


Research Article - (2024) Volume 2, Issue 3
A Scoping Review Involving Six English-Language Searches of COVID-19 Vaccine Hesitancy in Japanese Healthcare Providers Limited to Peer-Reviewed Publications
Received Date: Oct 07, 2024 / Accepted Date: Nov 05, 2024 / Published Date: Nov 28, 2024
Copyright: ©©2024 Carol Nash. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nash, C. (2024). A Scoping Review Involving Six English-Language Searches of COVID-19 Vaccine Hesitancy in Japanese Healthcare Providers Limited to Peer-Reviewed Publications. COVID Res OA, 2(3), 01-12.
Abstract
A recent publication regarding a March 2023 Google Scholar search found Japan unique in healthcare providers’ reaction to COVID-19 vaccines, with negative sentiment by healthcare providers toward vaccines defining the research in this area and concerns about side effects outweighing worries regarding infection. This current study investigates the anomaly through a scoping review of “COVID-19, Japan, vaccine hesitancy” in English-language peer-reviewed publications of six searches: Cochrane COVID-19 Study Register, OVID, ProQuest, PubMed, Scopus, and Web of Science. By following PRISMA guidelines, the intent is a more thorough examination of this unusual evaluation of COVID-19 vaccines by Japanese healthcare providers than offered by the March 2023 search. The finding is that of the 997 returns, only four were relevant for assessment inclusion. Of these four, three, published in Vaccines, support vaccine hesitancy in Japanese healthcare providers and their becoming more so regarding a subsequent dose of the vaccine. One article published in BMJ Open did not find this. Yet, the design of none of the studies was specific to investigating vaccine hesitancy in Japanese healthcare providers, making the conclusion questionable. Suggested future research directions include investigating the primacy of those databases searched and the need for timeliness in examining COVID-19 anomalies.
Keywords
COVID-19, Japan, Vaccine Hesitancy, Healthcare Providers, Databases
Introduction
A recent publication [1] on COVID-19 coping [2] considered extraversion as one of the Big Five [3,4] personality traits most socially relevant concerning positive COVID-19 coping [5–9]. During the COVID-19 pandemic from 2020 [10] to 2023 [11], the virus appeared in various waves [12], producing a surge of infection. When and how many of these waves occurred differed by country [13]. In the March 2023 Google Scholar search of “COVID-19 coping extraversion [number] wave”, fourteen individual countries were searched, as well as Europe as a whole (Table 1). The number of waves compared was up to five [1]. For most countries, research regarding extraversion and coping began during the first wave of COVID-19 [14], and coping positively improved with subsequent COVID-19 waves [15] and with the introduction of vaccines in December 2020 [16]. The exceptions are Israel/Palestine and the United States—where the research on COVID-19 coping went from positive to neutral—and Norway, where public sentiment initially was positive and became negative [1]. The results for Japan were unique regarding research on vaccine hesitancy of healthcare providers. Only in Japan was a decrease in COVID-19 coping evident because healthcare providers questioned vaccines after their introduction. In the other countries searched, vaccine introduction reduced the perceived threat of COVID-19 for healthcare providers [17,18]. For Japan, by wave five, with the vaccination program well underway, negative results were surprisingly recorded in the search of research on healthcare providers limited to the English language [1,19].
Table 1. COVID-19 Coping Regarding Extraversion—Described by Research as Predominantly Positive (+), Negative (−), or Neutral (o) Where the Period Defining a Wave Differs for Each Country and by Wave 4 (December 2020), Vaccines for COVID-19 Were Available in All Countries (Adapted from Table 3 in [1]—a Publication by this Author)
|
Country |
Wave 1 |
Wave 2 |
Wave 3 |
Wave 4 |
Wave 5 |
|
Austria |
o |
o |
|
|
|
|
Canada |
|
+ |
|
|
|
|
China |
|
+ |
+ |
|
+ |
|
Europe |
|
o |
|
|
|
|
Germany |
− |
o |
+ |
|
|
|
Greece |
o |
|
|
|
|
|
Iran |
|
|
|
+ |
+ |
|
Israel/Palestine |
+ |
o |
|
|
|
|
Italy |
+ |
|
|
|
|
|
Japan |
|
|
|
+ |
− |
|
Norway |
+ |
|
− |
|
|
|
Russia |
o |
|
|
|
|
|
Slovakia |
o |
+ |
|
|
|
|
United Kingdom |
− |
+ |
+ |
+ |
+ |
|
United States |
+ |
o |
|
|
|
This unanticipated result in association with the research on COVID-19 coping and extraversion for healthcare providers in Japan coincided with the particular introduction of vaccines in Japan—vaccines were introduced later in this country than in other countries because supply and bureaucratic problems created challenges with vaccine procurement and distribution [20]. Yet, irrespective of these difficulties, during the initial introduction of vaccines in Japan in the fourth COVID-19 wave, there was no identification of vaccine hesitancy in healthcare providers [20]. However, by the fifth wave of the pandemic, negative sentiment toward vaccines by those caring for COVID-19 patients focused scientific research in this area, with concerns about side effects from one vaccine (AstraZeneca) outweighing fears of infection [21].
The following study aims to investigate the extent of this anomaly in Japanese healthcare providers regarding COVID-19 vaccine hesitancy through a scoping review of “Japan COVID-19 vaccine hesitancy” restricted to English-language peer-reviewed publications undertaken following PRISMA guidelines [22]. As a scoping review of English-language peer-reviewed publications, it does not include non-peer-reviewed publications in any language or potentially relevant Japanese-language peer-reviewed sources. The reason is to follow the original limited review of the fourteen countries that searched only English-language peer- reviewed publications. Thus, this study has a less extensive aim than discovering all evidence regarding COVID-19 vaccine hesitancy in Japanese healthcare providers. Instead, it is to provide a more thorough assessment of English-language peer-reviewed publications of this unusual research result regarding the negative reconsideration of COVID-19 vaccines by healthcare providers in Japan. In this regard, there are two research questions.
Q1 According to the research published in English-language peer-reviewed journals, did Japanese healthcare providers develop increasing vaccine hesitancy over subsequent COVID-19 pandemic waves?
Q2 If so, what was the reason?
Materials and Methods
There is no published guidance on the necessary number of databases to search for a scoping review other than to advise that at least one database should be searched [23]. However, to provide the most extensive reach for this scoping review, the six searches include one register and five databases relevant to healthcare (Cochrane COVID-19 Study Register, ProQuest, PubMed, OVID, Scopus, and Web of Science)—databases considered to return consistent results irrespective of the date of the search, unlike Google Scholar [24].
Developed is a PRISMA flow of information diagram specific to scoping reviews based on the most recent PRISMA template [25], including the PRISMA Scoping Review Checklist in a supplementary file (Table S1) that outlines the review process. PRIMSA guidelines for scoping reviews are followed [26]. The recommendation is for researchers to use the PRISMA guidelines when completing the scoping review [26]. No registered review protocol exists for this scoping review.
As a COVID-19 investigation, the International Prospective Register of Systematic Reviews (PROSPERO) guidelines are relevant [27]. When the research question addresses the feasibility, appropriateness, meaningfulness, or effectiveness of a treatment or practice [28], a systematic review is advised—usually including a meta-analysis [29]. As this study instead identifies the extent of research available on a search of “COVID-19, Japan, vaccine hesitancy”, it is a scoping review rather than a systematic review [28], and registration with PROSPERO is thus not permitted [30].
“COVID-19, Japan, vaccine hesitancy” were the keywords searched for the one register and each database. The specific inclusion criteria beyond the PRISMA guidelines were that the returned reports be (1) published after the December 2020 availability of COVID-19 vaccines, (2) peer-reviewed, (3) written in English, and (4) include all of the searched terms regarding healthcare providers within the body of the text, Those excluded reports were (1) published before December 2020, (2) not peer- reviewed, (3) not in English, and (4) lacked any of the keywords regarding healthcare providers or included them in the reference list alone.
The search of the following register and databases was on 10 July: Cochrane COVID-19 Study Register, OVID, ProQuest, PubMed,
Results
Figure 1 represents the results of the PRISMA search process.
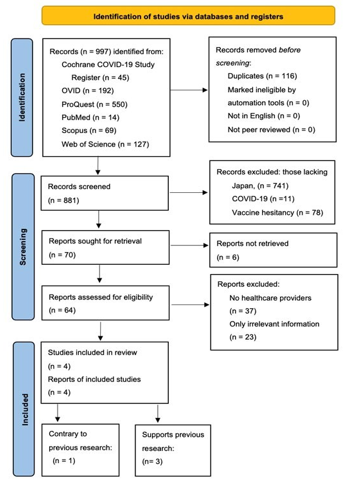
Figure 1. The PRISMA Flow of Information Chart [25] for a Search of the Parameter Containing the Keywords “COVID-19, Japan, Vaccine Hesitancy”, Conducted on 10 July 2024, of One Register and Five Primary Databases Relevant to Healthcare: Cochrane COVID-19 Study Register, OVID, Proquest, Pubmed, Scopus, and Web of Science.
Two subsections divide the results. The first corresponds to the various searches undertaken, providing commentary on conducting these types of searches. The second regards the articles returned that met all the criteria for inclusion.
Searches
The databases selected to search are those relevant to healthcare considered well-suited to meeting PRISMA guidelines—they are found suitable for their coverage and high precision of the search query, including their reproducibility of search results [31]. Consequently, it is relevant to consider whether the results from the searches performed substantiate this view of their suitability as search engines. The investigation will regard the number and type of returns for the searches of each database (see Table 2).
Table 2. Breakdown by Number of Returns Regarding Reasons for Excluding Returns of the Six Databases Searched for “COVID-19, Japan, Vaccine Hesitancy” on 10 July 2024, resulting in the Final Number of Included Articles—History of the PRISMA Exclusion Process is from Left to Right Regarding the Category Headings
|
Database |
Total Returns |
Duplicates |
No Japan |
No COVID-19 |
No vaccine hesitancy |
Not retrieved |
No health providers |
Irrelevant information |
Total included |
|
Cochrane |
45 |
42 |
|
|
|
2 |
|
1 |
0 |
|
OVID |
192 |
4 |
187 |
|
|
|
1 |
|
0 |
|
ProQuest |
550 |
11 |
520 |
1 |
10 |
|
7 |
1 |
0 |
|
PubMed |
14 |
4 |
9 |
|
1 |
|
|
|
0 |
|
Scopus |
69 |
55 |
|
4 |
9 |
|
|
1 |
0 |
|
Web of Science |
127 |
|
25 |
6 |
39 |
4 |
29 |
20 |
4 |
|
Total |
997 |
116 |
741 |
11 |
59 |
6 |
37 |
23 |
4 |
The Cochrane COVID-19 Study Register is a database of only COVID-19-related publications. Of the 45 returns, 42 were duplicates—all, except for two, in Web of Science. The two not duplicated in Web of Science were duplicated in ProQuest. Most of the results also returned in the Scopus search as well. Four Of those that are duplicates appear in Table S2. Three articles were not duplicating; two were unretrievable. The one retrievable contained irrelevant information regarding the search criteria. Although there were no returns unique to this search that were relevant to this investigation—of the duplicated returns—two are part of the included articles.
The initial search of the three keywords in the OVID database resulted in no returns. To improve the possibility of producing returns, “vaccine hesitancy” was removed from the search (also limited to English language and human). This modified search produced 192 results. Japan was not part of 187 of these returns, although it was one of the two keywords. Four returns were duplicates (ultimately, ones not part of the final list), and the remaining report did not include healthcare providers. The results were that none of the returns of this modified search produced any relevant studies.
The ProQuest search offered the most returns at 550 because the search engine retained articles that did not include Japan— remaining true even after modification to the parameter included the following limitations: not Malaysia, not India, not Thailand, not Italy, not China, not Hong Kong. These additional limitations produced the same number of returns with the same articles from Malaysia, India, Thailand, Italy, China, and Hong Kong (among studies of other countries). The initial search was on 10 July. For a search on 11 July, the number of returns increased to 778, while a search on 12 July reduced the returns to 700. The author analyzed the returns from 10 July, as the increase in the returns over subsequent days was unlikely relevant material. Of the 550 returns, 520 did not mention Japan. There were 11 duplicates with either Scopus or Web of Science (or both). Unlike the Cochrane COVID-19 Study Register or the OVID searches, some returns did not include COVID-19 (1) or vaccine hesitancy (10). Of the eight that remained, seven didn’t include healthcare providers, and of the one that did, it was irrelevant information. The final result was that there were no articles relevant to the considerations of this study.
Apart from OVID, PubMed produced the smallest number of returns at fourteen. Of these, nine were missing Japan. There were four duplicates and one not including vaccine hesitancy, resulting in no returns relevant to this investigation. Of the four duplicates, none were included.
For the Scopus search, there were 69 returns. There were 55 duplicates; 54 were with Web of Science and one with ProQuest. Like ProQuest, there were returns with no COVID-19 (4) or no vaccine hesitancy (9). The remaining unique return contained irrelevant information. Two reports relevant for consideration from the Web of Science were those in Scopus—the same publications duplicated in the Cochrane COVID-19 Study Register.
The Web of Science return represents the reference for the duplicated returns, providing the reason it includes no duplicates. There were 127 returns. Web of Science was the only database for which exclusions are under every category: no Japan (25), no COVID-19 (6), no vaccine hesitancy (39), not retrieved (4), no healthcare providers (29), and irrelevant information (20). Three studies eliminated were irrelevant because they tested vaccine hesitancy in healthcare providers at only one time point [32–34]. It is the only database producing exclusions in each category resulting from eliminating duplicates before all other considerations. Other searches would have produced exclusions in additional categories had this not been the process. The duplicate elimination process follows the PRISMA flow of information chart method [26].
Relevant Returns
Table 3 lists the relevant returns with their citation numbers and provides a breakdown of the search engines that produced them. There are four relevant articles. Web of Science returned all four. Cochrane COVID-19 Study Register and Scopus returned two.
Table 3. Articles Included from the Initial Search Of “COVID-19, Japan, Vaccine Hesitancy” Plus the Returns Including Healthcare Providers and if the Information in the Study was Relevant, Noting the Search Engines Returning the Articles, and Whether the Study Supports Japanese Healthcare Providers Becoming Increasingly Hesitant Regarding COVID-19 Vaccines
|
Article Title [citation #] |
Cochrane COVID-19 |
Scopus |
Web of Science |
Supports Research |
|
Association of Vaccine Confidence and Hesitancy in Three Phases of COVID-19 Vaccine Approval and Introduction in Japan [35] |
X |
X |
X |
Yes |
|
Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? [36] |
|
|
X |
Yes |
|
COVID-19 Vaccine hesitance and vaccine passports: a cross-sectional conjoint experiment in Japan [37] |
|
|
X |
No |
|
Differences in COVID-19 Vaccine Acceptance, Hesitancy, and Confidence between Healthcare Workers and the General Population in Japan [38] |
X |
X |
X |
Yes |
|
Total |
2 |
2 |
4 |
4 |
Of the relevant returns, there were three to which the answer to Q1—According to the research published in English-language peer-reviewed journals, did Japanese healthcare providers develop increasing vaccine hesitancy over subsequent COVID-19 pandemic waves?—is “Yes” [35,36,38] and one that is “No” [37].
Two articles by the Cochrane COVID-19 Study Register and Scopus returns are the same. These search engines returned only articles supporting earlier research that Japanese healthcare providers developed increasing vaccine hesitancy over subsequent pandemic waves. Web of Science was the sole search engine that returned an article contrary to this previous research.
Table 4 identifies that all the articles were published either in 2021 or 2022. There were no returns of assessment of vaccine hesitancy in Japanese healthcare providers regarding a more recent date. Considering those publications that supported the understanding of Japanese healthcare providers becoming increasingly hesitant about COVID-19 vaccines over subsequent waves, it is evident that these publications were in journals devoted to vaccines. The one return that provided information contrary to the view that Japanese healthcare providers became increasingly hesitant over subsequent pandemic waves concerning COVID-19 vaccines was a medical journal.
Table 4. Articles from Table 3 Listing The Date of Publication and the Publication Journal with the Journal Title in Italics Indicating the Article Lacking Support for Japanese Healthcare Providers Developing Increasing Vaccine Hesitancy
|
Article Title [citation #] |
Date |
Journal |
|
Association of Vaccine Confidence and Hesitancy in Three Phases of COVID-19 Vaccine Approval and Introduction in Japan [35] |
2022 |
Vaccines |
|
Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? [36] |
2021 |
Vaccines |
|
COVID-19 Vaccine hesitance and vaccine passports: a cross-sectional conjoint experiment in Japan [37] |
2022 |
BMJ Open |
|
Differences in COVID-19 Vaccine Acceptance, Hesitancy, and Confidence between Healthcare Workers and the General Population in Japan [38] |
2021 |
Vaccines |
The content of Table 5 includes each of the citation numbers of the relevant articles returned, plus the sample of the Japanese healthcare provider population surveyed, the design of the survey, and the type of outcome measurement. The results in this table indicate that, for each study, there was a relatively large sample of the Japanese healthcare provider population surveyed. Furthermore, all studies employed the same type of study design of a survey—some conducted online. Each report published in Vaccines used a Likert scale (four or five points). The article from BMJ Open relied on agreement or disagreement with pre-designed response options.
Table 5. Citation Numbers of Articles from Table 3, Population Studied, Study Design of Research, and the Outcome Measurement for each article Regarding COVID-19 Vaccine Hesitancy in Healthcare Providers Identified in Succeeding Waves of the Pandemic
|
# |
Japanese Healthcare Provider Population |
Study Design |
Outcome Measurement |
|
[35] |
7000 men and women, aged 20–80 |
web-based cross-sectional surveys |
“hesitancy” defined as not receiving at least one dose of vaccination survey time, and did not plan to do so in the future—5-point Likert scale |
|
[36] |
742 distributed questionnaires, 496 (294 males and 202 females) completed |
brief 15-item questionnaire survey |
Medical students rated their attitudes toward COVID-19 vaccination on a 4-point Likert scale |
|
[37] |
demographically representative sample of 5000 adults |
online survey |
To measure vaccine hesitancy, respondents were asked about their vaccination intentions, based on the response options: already vaccinated, willing to be vaccinated, undecided, and unwilling to be vaccinated. |
|
[38] |
1000 healthcare workers aged 20–69 years the target study population |
Survey explanation by e-mail, participants enrolled by e-mails, and apps until the target number was reached |
Hesitancy measurement by how many respondents agreed with the following statement: “When a vaccine for COVID-19 becomes available, I will get vaccinated.” A five-point Likert-type rating scale was used |
The content of Table 6 includes each of the citation numbers of the relevant articles returned plus a sample of the type of information published that identifies the article was either supportive or not of the March 2023 returns of the Google Scholar search concerning whether healthcare providers developed increasing vaccine hesitancy over successive COVID-19 waves. The information regarding procurement and distribution of specific vaccines, supplied in the two articles on Japan from the March 2024
Google Scholar search [20,21], was not mentioned in the relevant articles returned in this July 2024 scoping review. In contrast, the focus of the four articles returned in this scoping review is the direct relationship between the healthcare providers and their views on vaccines rather than the broader political context of the administration of vaccines in the country found included in the reports of the March 2024 Google Scholar search.
Table 6. Citation Numbers of Articles from Table 3 and COVID-19 Content Regarding Vaccine Hesitancy in Healthcare Providers Identified in Succeeding Waves of the Pandemic
|
[#] |
Relevant COVID-19 Content for Vaccine Hesitancy among Healthcare Providers |
|
[35] |
January 2021, before approval, 17.1% of healthcare providers vaccine hesitant; June 2021—start of elderly vaccination, 18.9% of healthcare providers vaccine hesitant; and September 2021—when vaccination was about 70% of the target population with at least one dose, 5.4% of healthcare providers show vaccine hesitancy. |
|
[36] |
Although most medical students (75.6%) stated that vaccines provide a high degree of protection against COVID-19, 67.3% were concerned about the sustainability of immunity by the vaccine. A non-negligible number of students (46.0%) stated that vaccine development was too rapid. |
|
[37] |
Healthcare workers, front-line essential workers, and those performing paid work were likely to be non-vaccine-hesitant compared with non-employed individuals: the former two groups were more likely to accept vaccination, showing ORs of 0.23 (95% CI 0.16 to 0.33) and 0.71 (95% CI 0.59 to 0.86), respectively. |
|
[38] |
Vaccine acceptance was higher among medical personnel attending patients with COVID-19, male healthcare workers, older healthcare workers, and doctors. The COVID-19 vaccine hesitancy rates were doctors, 11.7%; nurses, 18.5%; pharmacists, 17.1%; physical/occupational therapists, 13.8%. |
Results of the Four Articles
Association of Vaccine Confidence and Hesitancy in Three Phases of COVID-19 Vaccine Approval and Introduction in Japan [35] is one of the three returned articles published in the MDPI journal Vaccines. It represents the most relevant article of all the returns and was returned by three different databases (Cochrane COVID-19 Study Register, Scopus, and Web of Science), investigating the vaccine hesitancy of Japanese healthcare providers over three periods. This research is a study of healthcare providers undertaken as part of a more comprehensive study of the views of Japanese citizens. In this investigation of 7000 citizens, healthcare providers represented 808 (11.2%) of those studied at T1, 824 (11.4%) at T2, and 830 (11.5%) at T3. The three separate interviews were in January 2021, before vaccine approval; in June, the start of elderly vaccination; and in September, with vaccination of approximately 70% of the target population with at least one dose, when vaccine hesitancy for the total population was 17.5%, 65.3%, and 19.4%, respectively. Thus, for the total population, vaccine hesitancy continued and peaked in June. From this perspective, the vaccine hesitancy of healthcare providers, although following the same trend of a higher percentage of vaccine hesitancy in June, was comparatively low at 17.1%, 18.9%, and 5.4% in these three intervals. This trend reveals that in January, before vaccine approval, healthcare providers had almost the same vaccine hesitancy as the larger population. However, in June, when vaccine hesitancy by the general population escalated, the vaccine hesitancy of healthcare providers was kept down, with only a slight rise from the January results. There was the elimination of almost all vaccine hesitancy in healthcare providers by September—when vaccine hesitancy by the general population was higher than before vaccines were approved.
Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? [36], represents the second article noting an increase in vaccine hesitancy of healthcare providers published in Vaccines. It was returned only by Web of Science. Published on 8 November 2021, the time from submission of this manuscript to its publication is only one month. Unlike the previous article in Vaccines, this study did not test Japanese medical students at different periods. Making this study still relevant is that the research asked medical students who had received the second dose of the vaccine whether they would be willing to receive the third dose. Among all the participants, 89.1% (442/496) received the second dose of the vaccine, and 84.5% (419/496) of the participants were willing to receive a third dose. Although this was a hypothetical response, it is clear that fewer medical students were willing to receive the third dose than had received the second dose. Although most of the students (75.6%; 375/496) agreed that the vaccines provide a high degree of protection against COVID-19, 67.3% (334/496) were concerned about the sustainability of immunity by the vaccine. A non-negligible number of medical students (46.0%; 228/496) stated that the vaccine development was too rapid.
COVID-19 Vaccine hesitance and vaccine passports: a cross- sectional conjoint experiment in Japan [37] is the only article returned that did not find an increase in vaccine hesitancy among healthcare providers. Returned solely by Web of Science, this article is also unique to those returned in being published in a medical journal, BMJ Open, rather than one devoted to vaccines. Compared to the others, acceptance of this article for publication was the longest. The submission is on 6 January 2022, and the acceptance is on 1 June 2022. Healthcare providers were among the sample of 5000 Japanese adults for this study. Healthcare providers represented 6.4% of those studied or 320 participants. The first part of this study of 5000 occurred from 21 July 2021 to 23 July 2021; the follow-up study was between 10 November 2021 and 20 November 2021, including 4367, or 87.3% of those participating in the original investigation. The authors do not provide a breakdown of the percentage of healthcare providers who participated in the second part of the study; they add healthcare providers with essential workers without providing the change in vaccine hesitancy but generally claim they are less likely to be vaccine-hesitant. The article indicates that when healthcare providers are vaccine-hesitant, the factors are side effects, safety, and vaccine mistrust. Without the article's specific focus on healthcare providers in the second period, a comparison is difficult of this publication that did not find an increase in vaccine hesitancy with the subsequent pandemic wave with the others that did.
Differences in COVID-19 Vaccine Acceptance, Hesitancy, and Confidence between Healthcare Workers and the General Population in Japan [38] is the third article published in Vaccines. It was received by the journal on 22 October 2021, revised on 12 November 2021, accepted on 18 November 2021, and published on 24 November 2021. Among a more extensive investigation of vaccine hesitancy in the Japanese population, this study looked at vaccine hesitancy in healthcare providers. The first period examined was pre-COVID-19—when Japan had one of the lowest vaccine acceptance rates in the world [39]. The authors differentiated healthcare providers from the general population based on these results, including physicians, nurses, pharmacists, and physical and occupational therapists, as part of their study among the 755 healthcare providers (medical clerks make up the additional 275 participants in the total of 1030 healthcare workers). The results of vaccine hesitancy follow—general population, 17.5%; doctors, 11.7%; nurses, 18.5%; pharmacists, 17.1%; physical/occupational therapists, 13.8%. Female sex, younger age, being a nurse, influenza vaccine hesitancy, and concern about the frequency of adverse events were positively associated with vaccine hesitancy in the study. Although this study did investigate vaccine hesitancy at two points, the first was pre-COVID-19, and the second was before the vaccine was available; therefore, the usefulness of these results for this current study is limited.
Discussion
This study is in response to a previous English-language Google Scholar search of peer-reviewed publications during March 2023 that identified Japan as unique in its healthcare providers developing increased COVID-19 vaccine hesitancy in subsequent waves of the pandemic. The purpose was to determine if this held in other studies from an English-language search of peer-reviewed publications regarding “COVID-19, Japan, vaccine hesitancy”, and, if so, why this might be the case. The original research had identified healthcare providers as developing increased vaccine hesitancy between wave four and wave five [19]. Further research in [1] speculated that the reason for this vaccine hesitancy in Japan might be the negative sentiment of the general public toward vaccines that dominated, with concerns about side effects from AstraZeneca in particular outweighing fears of infection [21]. For this reason, the consideration was that a fuller investigation of vaccine hesitancy in Japanese healthcare providers was warranted.
An extensive search of six relevant databases produced a return of 997 articles. In following the PRISMA guidelines, only four articles remained from these returns. Three of these articles supported the view that over subsequent waves, healthcare providers developed increasing vaccine hesitancy [35,36,38]. Publication of each of these articles is in Vaccines. The one article presenting a contrary assessment [37] is in the medical journal BMJ Open. Yet, those articles that supported the view that healthcare providers grew increasingly vaccine hesitant did not undertake to study their vaccine hesitancy—the information can be identified by looking through each article for the necessary result—the consequence is that the information lacks clarity. Only the first paper [35] specifies that between January (before the introduction of vaccines in Japan) and June, there was an increase in vaccine hesitancy in healthcare providers—but the increase was a slight 1.8%. The vaccine hesitancy of the second supporting paper [36] was purely hypothetical regarding whether medical students would be inclined to get a third dose of the vaccine after receiving the second. The final paper that supports healthcare providers became increasingly vaccine hesitant [38], although it tests for two different times regarding vaccine hesitancy, one of these times is before COVID-19. Thus, its report of increased vaccine hesitancy for this study becomes irrelevant. The weakness of one paper that presented contrary information on vaccine hesitancy in healthcare providers [37] is that it provides incomplete results regarding the second testing time of healthcare providers. This study reported on many variables over the two time periods, with healthcare providers being only one. The authors of this study chose to provide less information concerning the vaccine hesitancy of healthcare providers; therefore, the ability to determine why this research did not find the same trend as others is unknown.
Regarding the two research questions:
Q1 According to the research published in English-language peer-reviewed journals, did Japanese healthcare providers develop increasing vaccine hesitancy over subsequent COVID-19 pandemic waves?
Q2 If so, what was the reason?
The outcome from this scoping review of English-language peer- reviewed journals found that, although there is some, there is little evidence that there was increasing vaccine hesitancy in Japanese healthcare providers over subsequent COVID-19 pandemic waves. Furthermore, the evidence provided is not available from medical journals—it is from one journal devoted to vaccines. There is no direct evidence regarding the reason for vaccine hesitancy among these healthcare providers. Consequently, there is no definitive answer to Q2 available. From [35], healthcare providers were vaccine hesitant because this was the predominant view of the larger population. Regarding [36], if healthcare providers were vaccine hesitant, it was because of a concern about the sustainability of immunity by the vaccine in considering vaccine development too rapid. There can be no explanation of the reason from [38] as the two time periods examined were pre-vaccine.
The strengths of this review are that it is a complete scoping review rather than a limited review. The presentation of this scoping review is in exceptional detail, following the scoping review guidelines of PRISMA. The author actively undertook—and accomplished—including all relevant databases in this scoping review. This research is significant in being the first to undertake a scoping review of English-language peer-reviewed publications to identify the research concerning this matter as, to the best of the author’s knowledge, there are no other studies in English-language peer-reviewed journals on vaccine hesitancy among Japanese healthcare providers during the COVID-19 pandemic.
Limitations
In a scoping review, researchers map, describe, and analyze a wider body of literature than a systematic review while following a more rigorous method than traditional narrative literature reviews, but at the cost of the meticulousness of systematic reporting guidelines. Although the PRISMA extension for scoping reviews provides a recommended framework for methodological issues [26], it falls short of offering any consistent approach to the specifics of charting and synthesis [40]. Therefore, following the PRISMA guidelines for this scoping review is a limitation of this research.
The study limitations primarily pertain to the lack of information available from a scoping review of English-language peer-reviewed journals in answering the research questions confidently. Although there may be additional information from grey literature [41] and Japanese-language sources to answer the two research questions, this is a scoping review of English language peer-reviewed articles alone—a limitation to finding out what happened during that time in Japan. Of the reports returned, a partial answer responds to the first research question—three studies recognize an increase in vaccine hesitancy in healthcare providers over subsequent waves; however, the data are not convincing for the reasons provided. The studies investigated did not provide the reason because it was uninvestigated—answering the second research question. Furthermore, studies regarding general vaccine hesitancy in Japan are in contradiction. The research in [35] resulted from a pre- COVID-19 survey of over 280,000 people in 149 countries and regions—it found Japan with one of the lowest rates of vaccine confidence. Yet, another of the returns from the Web of Science— excluded from consideration as not meeting all the study criteria— states the opposite and found worldwide that Japan has one of the highest public acceptance rates for the COVID-19 vaccine [42]. The Japanese problem with the AstraZeneca vaccine noted in [19] is not part of any other publication.
More specifically, a limitation of this study is that the searches were of only English-language peer-reviewed publications. Restricting the searches this way corresponds with the March 2024 publication that initiated this study and had similar restrictions. Still, within these search constraints, it was impossible to understand the extent of COVID-19 vaccine hesitancy in Japanese healthcare providers and to find compelling results for why these healthcare providers may have become COVID-19 vaccine-hesitant.
Cognitive bias is a possibility, with the conducting of research independently by one researcher [43,44]. Although the author intended to be unbiased concerning this assessment, the author could be unaware of having cognitive bias during the examination. The author has included the record provided by the database of reports returned for each search conducted as one aspect to mitigate cognitive bias. These records are in Table S2. Creating a detailed color-coded system helped to identify and differentiate articles following the PRISMA process. All considered returns include those articles retrievable. Then, an inspection of their content eliminated irrelevant articles. Differentiated were those presenting a view contrary to Japanese healthcare providers demonstrating increasing vaccine hesitancy and those reports corresponding to this view. Quotations from each potentially relevant article appear on List S1 so that the author’s reasons for making the judgment concerning each report for inclusion are evident and can be confirmed. By taking these precautions, the author actively intended to alleviate cognitive bias.
Future Research Directions
In considering future research in this area, the time has now passed to research the vaccine hesitancy among healthcare providers in subsequent waves of COVID-19. Some research found that the healthcare providers in Japan behaved differently than in other countries. There was reason at that time to investigate this further, work undone in English-language peer-reviewed publications. Consequently, there was a missed research opportunity. However, in considering the results of the searches performed, future research can investigate the suitability of various databases as primary.
One of the reasons Google Scholar is not considered suitable as a primary database [31] but acceptable for grey literature searches [45] is that returns are inconsistent [24]. Future research should reinvestigate the results that have judged Google Scholar as particularly deficient as a primary database, especially since its returned results are substantial, and ProQuest is not questioned as a database for primary searches [46]. With consistency as a criterion, if there is good reason for continuing to assess Google Scholar as inappropriate as a primary database, reconsideration should be given to ProQuest as a primary database, resulting from the return of 550 articles one day, 778 the next, and 700 on the third for this study. Additionally, problematic is that the ProQuest returns did not eliminate other countries from consideration even when specifically mentioned for exclusion in the search.
What is also relevant concerning the health-related databases— OVID and PubMed—is that neither was appropriate for investigating vaccine hesitancy among healthcare providers. Only the science databases were valuable in this regard. The Cochrane COVID-19 Study Register, Scopus, and Web of Science returns were similar in most respects. However, there were some differences. Future research can investigate the considerations that permit these databases to return similar results and what aspects produce differences.
There is a twofold impact on the scientific community regarding the results of this study. The first is that investigation of recognized country anomalies regarding vaccine hesitancy in pandemics should be when results are obtainable. It is insufficient to examine this outcome once a pandemic is over. The second—pandemic researchers should be aware that English-language medical journals may provide little relevant information regarding vaccine hesitancy. To this point, more journals should publish studies on vaccine hesitancy in healthcare providers than Vaccines alone. These changes would improve the ability of the scientific community to make recommendations on vaccine hesitancy in healthcare providers. As vaccine hesitancy in healthcare providers is identified as the most significant reason for vaccine hesitancy in the general population [47], improving research on vaccine hesitancy in healthcare providers is valuable in controlling future pandemics.
Conclusion
The research questions of this study are two. Did Japanese healthcare providers develop increasing vaccine hesitancy over subsequent COVID-19 pandemic waves? If so, what was the reason? The scoping review of six relevant databases produced 997 returns, with only four included. Of those four, three supported that Japanese healthcare providers developed increasing vaccine hesitancy. However, this development was slight, and the data were insufficiently robust for a conclusive assessment. An inability to usefully assess the results also hampered the one article that provided a contrary point of view. None of the articles included considered the reason for vaccine hesitancy among healthcare providers. This study highlights the necessity of timely research when unexpected anomalies occur regarding COVID-19 and the value of ensuring databases are appropriate and reliable.
Supplementary Materials: The following supporting informa- tion can be downloaded: https://zenodo.org/records/14184606 Table S1: Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-SCR) Checklist, Table S2. Report title, database returning the report, re- port date, and report inclusion status.
Funding: This research received no external funding.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: Not applicable.
Data Availability Statement: No new data were created.
Conflicts of Interest: The author declares no conflicts of interest.
References
- Nash, C. (2023). Extraversion in COVID-19 Coping and Actionable Insights from Considering Self-Directed Learning. COVID, 3(6), 831-858.
- Kar, N., Kar, B., & Kar, S. (2021). Stress and coping during COVID-19 pandemic: Result of an online survey. Psychiatry research, 295, 113598.
- Zeigler-Hill, V., & Shackelford, T. K. (Eds.). (2020). Encyclopedia of personality and individual differences. Cham: Springer International Publishing.
- Anglim, J., Horwood, S., Smillie, L. D., Marrero, R. J., & Wood, J. K. (2020). Predicting psychological and subjective well-being from personality: A meta-analysis. Psychologicalbulletin, 146(4), 279.
- Gashi, D., Gallopeni, F., Imeri, G., Shahini, M., & Bahtiri,S. (2023). The relationship between big five personality traits, coping strategies, and emotional problems through the COVID-19 pandemic. Current Psychology, 42(33), 29179-29188.
- Wang, C., Havewala, M., & Zhu, Q. (2024). COVID-19stressful life events and mental health: Personality and coping styles as moderators. Journal of American College Health, 72(4), 1068-1077.
- Xie, C. S., & Kim, Y. (2022, January). Post-traumatic growth during COVID-19: The role of perceived social support, personality, and coping strategies. In Healthcare (Vol. 10, No. 2, p. 224). MDPI.
- NikÄeviÄ?, A. V., Marino, C., Kolubinski, D. C., Leach, D., & Spada, M. M. (2021). Modelling the contribution of the Big Five personality traits, health anxiety, and COVID-19 psychological distress to generalised anxiety and depressive symptoms during the COVID-19 pandemic. Journal of affective disorders, 279, 578-584. 9.
- Gibbons, C. (2022). Understanding the role of stress, personality and coping on learning motivation and mental health in university students during a pandemic. BMC psychology, 10(1), 261.
- Cucinotta, D., & Vanelli, M. (2020). WHO declares COVID-19 a pandemic. Acta bio medica: Atenei parmensis, 91(1), 157.
- Rigby, J., & Satija, B. (2023). WHO declares end to COVID global health emergency. Reuters: London, UK.
- Ayala, A., Villalobos Dintrans, P., Elorrieta, F., Castillo, C., Vargas, C., & Maddaleno, M. (2021). Identification of COVID-19 waves: considerations for research and policy. International Journal of Environmental Research and Public Health, 18(21), 11058.
- Swain, R. B., Lin, X., & Wallentin, F. Y. (2024). COVID-19pandemic waves: Identification and interpretation of global data. Heliyon, 10(3).
- Pilch, I., Wardawy, P., & Probierz, E. (2021). The predictors of adaptive and maladaptive coping behavior during the COVID-19 pandemic: The Protection Motivation Theory and the Big Five personality traits. PLoS One, 16(10), e0258606.
- Rogowska, A. M., KuÅ?nierz, C., & Ochnik, D. (2021). Changes in stress, coping styles, and life satisfaction between the first and second waves of the COVID-19 pandemic: A longitudinal cross-lagged study in a sample of university students. Journal of Clinical Medicine, 10(17), 4025.
- Lamb, Y. N. (2021). BNT162b2 mRNA COVID-19 vaccine:first approval. Drugs, 81, 495-501.
- Tavilani, A., Abbasi, E., Ara, F. K., Darini, A., & Asefy,Z. (2021). COVID-19 vaccines: Current evidence and considerations. Metabolism open, 12, 100124.
- Koltai, J., Raifman, J., Bor, J., McKee, M., & Stuckler, D. (2022). COVID-19 vaccination and mental health: a difference- in difference analysis of the understanding America study. American Journal of Preventive Medicine, 62(5), 679-687.
- Odachi, R., Takahashi, S., Sugawara, D., Tabata, M.,Kajiwara, T., Hironishi, M., & Buyo, M. (2022). The Big Five personality traits and the fear of COVID-19 in predicting depression and anxiety among Japanese nurses caring for COVID-19 patients: A cross-sectional study in Wakayama prefecture. Plos one, 17(10), e0276803.
- Lipscy, P.Y. (2023) Japan’s Response to the COVID-19 Pandemic. In Japan Decides 2021: The Japanese General Election ( pp. 239–254). Cham: Springer International Publishing.
- Niu, Q., Liu, J., Kato, M., Shinohara, Y., Matsumura, N., Aoyama, T., & Nagai-Tanima, M. (2022). Public opinion and sentiment before and at the beginning of COVID-19 vaccinations in Japan: Twitter analysis. JMIR infodemiology, 2(1), e32335.
- Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., ... & Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of internal medicine, 169(7), 467-473.
- Peters, M. D., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., ... & Khalil, H. (2020). Updated methodological guidance for the conduct of scoping reviews. JBI evidence synthesis, 18(10), 2119-2126.
- Gusenbauer, M. (2019). Google Scholar to overshadow them all? Comparing the sizes of 12 academic search engines and bibliographic databases. Scientometrics, 118(1), 177-214.
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I.,Hoffmann, T. C., Mulrow, C. D., ... & Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. bmj, 372.
- McGowan, J., Straus, S., Moher, D., Langlois, E. V., O'Brien,K. K., Horsley, T., ... & Tricco, A. C. (2020). Reporting scoping reviews—PRISMA 2020 2024. Journal of clinical epidemiology, 123, 177-179.
- Farrah, K., Young, K., Tunis, M. C., & Zhao, L. (2019). National Institute for Health and Care Research International Prospective Register of Systematic Reviews. PROSPERO 2020, 8, 1-9.
- Munn, Z., Peters, M. D., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC medical research methodology, 18, 1-7.
- Campbell, M., McKenzie, J. E., Sowden, A., Katikireddi,S. V., Brennan, S. E., Ellis, S., ... & Thomson, H. (2020). Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. bmj, 368.
- National Institute for Health and Care Research International Prospective Register of Systematic Reviews. PROSPERO 2020.
- Gusenbauer, M., & Haddaway, N. R. (2020). Which academic search systems are suitable for systematic reviews or metaâ? analyses? Evaluating retrieval qualities of Google Scholar, PubMed, and 26 other resources. Research synthesis methods, 11(2), 181-217.
- Suzuki, N., Yamamoto, T., Uchiumi, C., & Sugaya, N. (2022). Socio-economic and behavioral characteristics associated with COVID-19 vaccine hesitancy under a declared state of emergency in Japan. Brain, Behavior, & Immunity-Health, 22, 100448.
- Takahashi, S., Takahashi, N., Sasaki, S., Nohara, M., & Kawachi, I. (2022). Occupational disparities in COVID-19 vaccine hesitancy in Japan. SSM-population health, 19, 101226.
- Ghaznavi, C., Yoneoka, D., Kawashima, T., Eguchi, A., Murakami, M., Gilmour, S., ... & Nomura, S. (2022). Factors associated with reversals of COVID-19 vaccination willingness: Results from two longitudinal, national surveys in Japan 2021-2022. The Lancet Regional Health–Western Pacific, 27.
- Tokiya, M., Hara, M., Matsumoto, A., Ashenagar, M. S., Nakano, T., & Hirota, Y. (2022). Association of vaccine confidence and hesitancy in three phases of COVID-19 vaccine approval and introduction in Japan. Vaccines, 10(3), 423.
- Sugawara, N., Yasui-Furukori, N., Fukushima, A., & Shimoda,K. (2021). Attitudes of medical students toward COVID-19 vaccination: who is willing to receive a third dose of the vaccine?. Vaccines, 9(11), 1295.
- Okamoto, S., Kamimura, K., & Komamura, K. (2022). COVID-19 vaccine hesitancy and vaccine passports: a cross- sectional conjoint experiment in Japan. BMJ open, 12(6), e060829.
- Hara, M., Ishibashi, M., Nakane, A., Nakano, T., & Hirota,Y. (2021). Differences in COVID-19 vaccine acceptance, hesitancy, and confidence between healthcare workers and the general population in Japan. Vaccines, 9(12), 1389.
- De Figueiredo, A., Simas, C., Karafillakis, E., Paterson, P., & Larson, H. J. (2020). Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study. The Lancet, 396(10255), 898-908.
- Bradbury-Jones, C., Aveyard, H., Herber, O. R., Isham, L., Taylor, J., & O’malley, L. (2022). Scoping reviews: the PAGER framework for improving the quality of reporting. International Journal of Social Research Methodology, 25(4), 457-470.
- Mering, M. (2018). Defining and understanding grey literature.Serials Review, 44(3), 238-240.
- Takamatsu, A., Honda, H., Miwa, T., Tabuchi, T., Taniguchi, K., Shibuya, K., & Tokuda, Y. (2023). Factors associated with COVID-19 booster vaccine hesitancy: a nationwide, cross- sectional survey in Japan. Public Health, 223, 72-79.
- Neal, T., Lienert, P., Denne, E., & Singh, J. P. (2022). A general model of cognitive bias in human judgment and systematic review specific to forensic mental health. Law and human behavior, 46(2), 99.
- Halpern, S. D., Truog, R. D., & Miller, F. G. (2020). Cognitive bias and public health policy during the COVID-19 pandemic. Jama, 324(4), 337-338.
- Haddaway, N. R., Collins, A. M., Coughlin, D., & Kirk, S. (2015). The role of Google Scholar in evidence reviews and its applicability to grey literature searching. PloS one, 10(9),e0138237.
- Kraft, A. (2019). ProQuest One Academic. The Charleston Advisor, 21(1), 43-48.
- Biswas, N., Mustapha, T., Khubchandani, J., & Price, J. H.(2021). The nature and extent of COVID-19 vaccination hesitancy in healthcare workers. Journal of community health, 46, 1244-1251.