
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Case Report - (2017) Volume 2, Issue 2
A Ruptured Spontaneous Heterotopic Tubal Pregnancy With a Viable Intrauterine Pregnancy
2Cancer Biology program, Morehouse School of Medicine, Georgia Cancer Center for Excellence, Atlanta,, USA
Received Date: Jul 20, 2017 / Accepted Date: Jul 27, 2017 / Published Date: Aug 05, 2017
Copyright: ©Ashley Wiltshire, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
An ectopic pregnancy is a pregnancy located outside of the intrauterine cavity.They comprise 1-2% of all first trimester pregnancies and 6% of pregnancy related deaths in the United States [1]. Ectopic pregnancies most commonly occur in the fallopian tube but can also implant in other locations, including the ovaries, peritoneal cavity, cesarean section scars and the cervix [2].
Introduction
An ectopic pregnancy is a pregnancy located outside of the intrauterine cavity.They comprise 1-2% of all first trimester pregnancies and 6% of pregnancy related deaths in the United States [1]. Ectopic pregnancies most commonly occur in the fallopian tube but can also implant in other locations, including the ovaries, peritoneal cavity, cesarean section scars and the cervix [2].
Heterotopic pregnancy
A heterotopic pregnancy is when an intrauterine pregnancy and an extra uterine pregnancy occur simultaneously. Ninety percent involve simultaneous intrauterine and tubal gestations [2]. Spontaneous or naturally occurring heterotopic pregnancies are rare and are estimated to occur in 1:30,000 pregnancies [3]. For pregnancies conceived following ovulation induction, heterotopy is much more common at 0.5-1% [1]. The incidence of heterotopy for all pregnancies, naturally conceived and those utilizing artificial reproductive technology combined is approximately 1:7,000 [3].
Besides ART and ovulation induction, another common risk factor for ectopic pregnancies includes tubal disease. Tubal disease can be secondary to a history of sexually transmitted infections, such as chlamydia and gonorrhea, which are notoriously associated with pelvic inflammatory disease. There are also congenital anomalies, such as those related to DES exposure in utero, that are associated with malformed tubes [2]. Other abdominopelvic inflammatory conditions, such as endometriosis, appendicitis, peritonitis, and Crohns disease, can also lead to anatomical distortion of the fallopian tubes via progression of inflammation and adhesion formation. Lastly, prior surgical manipulation of the fallopian tubes through tubal sterilization, tubal sterilization reversal, and salpingostomy orsalpingoplasty for ectopic treatment can also increase the risk of ectopic pregnancy [1].
Due to its extreme rarity, heterotopic pregnancies are often very difficult to diagnose, especially when the patient lacks or denies risk factors. If the patient is hemodynamically stable, once an intrauterine pregnancy (IUP) is visualized the working diagnosis of a heterotopic pregnancy is commonly and quickly dismissed. This is consistent with many published suggested algorithms for the work up of a suspected ectopic pregnancy [1]. Unfortunately, symptoms of an un-ruptured heterotopic gestation can be masked by other seemingly more likely diagnoses such as round ligament pain, threatened/missed abortion and cervicitis. Often times, it is not until there is tubal rupture when hemodynamic instability presents, adding concrete direction in the assessment and diagnosis of an early heterotopic pregnancy. Approximately 70% of heterotopic pregnancies are diagnosed between 5-8 weeks, 20% between 9-10 weeks, and 10% after 11 weeks gestation [4].
Case
The clinical case is of a ruptured spontaneous heterotopic tubal pregnancy of a 30 year old G5P4004. The patient initially presented to the emergency department (ED) with severe and diffuse post-coital lower abdominal pain for 3-4 hours.She also endorsed shortness of breath, lightheadedness and persistent nausea and vomiting during the 4 days leading up to presentation. She was unsure of the date of her last menstrual period, but noted that she may have skipped 1-2 cycles. During the initial assessment, the patient was noted to be intermittently hypotensive (108-97/61-50), tachycardic (120s-130s bpm), diaphoretic, with worsening pallor and fluctuating mental status. AFocused Assessment with Sonography forTrauma scan revealedhemoperitoneum and an IUP with fetal cardiac activity [5].Leukocytosis was noted at 20.7 K/mcL. Initial hemoglobin and hematocrit was 10.9 g/dL and 32.6%, respectively
The differential diagnosis at this time included ruptured tubal heterotopic pregnancy vs. an acute abdomen due to gastroentrologic or vascular etiologies. All possible diagnoses were deemed highly unlikely by respective medical teams.A bedside trans-vaginal ultrasound and repeat abdominal US revealed an intrauterine gestational sac with a fetal pole measuring approximately 6 weeks, a yolk sac, fetal cardiac activity, free fluid in the pelvic cavity and free fluid in all abdominal quadrants up to the liver edge.
Due to the patients worsening hemodynamic stability, CT imaging was bypassed and the patient was taken straight to the operating room for exploratory laparotomy. The patient received 2 units of packed red blood cells (PRBCs) preoperatively. Surgical findings included 1,000 cc of hemoperitoneum, a ruptured left fallopian tube, a gravid uterus measuring approximately 6-8 week size, normal appearing right fallopian tube, and normal appearing bilateral ovaries and no evidence of adhesive disease. Total left salpingectomy was performed (Fig 1-2). Pathology analysis confirmed products of conception within the surgical specimen (Fig. 3-4).

Figure 1: The image above is during the process of coagulating and ligating the mesosalpinx of the affected fallopian tube with a Ligasure. The ruptured site is immediately distal to the most medial babcock. The gravid uterus is also pictured

Figure 2: The above image is of the left fallopian tube after salpingectomy. It is being measured from the isthmus to fimbriated end. The ruptured site is located at the 2 inch mark

Figure 3: Low power view of dilated fallopian tube lumen containing placental fragments and blood. These fragments are angioinvasive, eroding into the wall and vasculature of the fallopian tube wall.

Figure 4: High power magnification of intraluminal placental fragments consisting of chorionic villi with surface lined by a single layer of cytotrophoblasts and multinucleated scattered syncytiotrophoblasts admixed with blood.
The patient’s post-operative course was unremarkable. She received 1 unit of PRBCs post operatively. An official obstetrical ultrasound was performed on post-operative day (POD) #0 re-confirming the presence of a viable IUP, dated 6.1 weeks with a 2.4 cm sub chorionic bleed (Fig 5-6). The patient was discharged on POD#1. She went on to have a full term spontaneous vaginal delivery of the remaining IUP. Of note, upon chart review, it was noted that the patient was diagnosed with 2 separate episodes of gonorrhea and chlamydia, 6 and 11 years prior, respectively. Both infections had been treated and followed by a negative test of cure. The patient, upon the initial encounter in the ED, did not report this information. Due to the urgent nature of her presentation, she was not immediately assigned to her electronic medical chart, but instead received a temporary chart to allow for her immediate management.
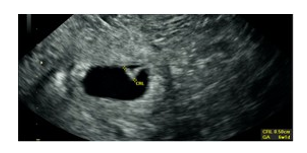
Figure 5: ultrasound imaging of the single IUP; Crown Rump Length is 0.5cm consistent with 6.1week gestational age with fetal cardiac activity of 113BPM
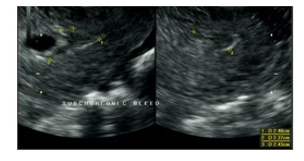
Figure 6: ultrasound imaging of 2.4cm sub-chorionic bleed
Conclusion
Management of tubal heterotopic pregnancies is commonly complicated by difficulties in diagnosis and the need to protect the co-existing IUP. Even though the presentation of a tubal heterotopic pregnancy is often similar to the average singleton tubal ectopic pregnancy, accurate diagnosis is usually derailed upon visualization of an IUP.Unfortunately, patient presentation to a health care provider may be delayed until significant acute physical signs and symptoms present, further delaying proper diagnosis and management. Essentially, this common quick disregard of a heterotopic diagnosis upon presentation can be life threatening to both the patient and the concurrent IUP.
Heterotopic pregnancies are typically managed surgically with salpingectomy or salpingostomy via laparoscopy or laparotomy. Deciding between laparoscopy vs. laparotomy should be based on the patients’ hemodynamic status, blood loss, and the surgical skill of the provider.When deciding between salpingostomy vs. salpingectomy, one should weigh the patient’s desire for future fertility, risk of a repeat ectopic in the future, and the risk of persistent ectopic pregnancy. Of note, it has been reported that up to 8% of tubal pregnancies treated with salpingostomiesresult in a persistent tubal pregnancy [4].This is of particular importance because persistent tubal pregnancies frequently result in tubal rupture, which, again, can be life threatening for the patient and further complicate the management of the concurrent IUP [2].
Other surgical management modalities reported in the literature include local injection of potassium chloride, hyperosmolar glucose, or methotrexate into the gestational sac laparoscopically or under ultrasound guidance4, 6.The body then reabsorbs the products of conception or theprocedure can be followed by aspiration of the tubal pregnancy [4,6]. Medical management with systemic methotrexate is not an option due to the concurrent IUP. Overall, the survival rate for the IUP after the tubal pregnancy is treated surgically has been reported to be between 35-54%, with a delivery rate of 66% [4]. We decided to perform a salpingectomy for this patient,due to the emergent nature of her presentation, her lack of desire for future fertility and to decrease her risk of repeat ectopic pregnancy in the future.
In conclusion, a high index of suspicion is imperative for timely management and successful obstetrical outcome, especially for those who lack or deny obvious risk factors.Despite the oftenemergent presentation of heterotopic pregnancies, surgical management with preservation of the intrauterine pregnancy, even after tubal rupture, is feasible and patients should be counseled accordingly.
Acknowledgements: Dr. Mario Mosunjac for providing histologic pictures. VNR’s lab was supported by Georgia Cancer Coalition Distinguished Cancer Scholar award, NIH-NCRR-RCMI grant G-12-RR003034, U54 RR02613, 5P20RR11104 and NIHMD research endowment grant 2S21MD000101, U54 CA118638 and by private funds from the VOYA foundation and It’s the Journey Inc.
References
- Cunningham G, Bradshaw K, Hoffman B, Halvorson L, Schaffer J, et al. (2014) Williams Obstetrics. 24th Ed. New York: McGraw-Hill Medical. Chapter 7, Ectopic Pregnancy 157-171
- Speroff L, Fritz, M. (2005) Clinical Gynecologic Endocrinology and Infertility. 8th ed. Philadelphia: Lippincott Williams & Wilkins; Chapter 13, Ectopic Pregnancy 1283-1412.
- MJ G, R R. (2008) Heterotopic pregnancy in natural conception. Journal of Human Reproductive Sciences. 1: 37-38.
- AarathiCholkeri-Singh, Ann LaBarge. (2007) Spontaneous heterotopic triplets: a case report. Fertility and Sterility 88: p968. e5-968.e7.
- Scalea T, Rodriguez A, Chiu W, Brenneman F, Fallon W, et al. (1999). “Focused Assessment with Sonography for Trauma (FAST): results from an international consensus conference”. Journal of Trauma. 46: 466-472.
- Chadee A, Rezai S, Kirby C, Ekaterina Chadwick, Sri Gottimukkala, et al. (2016). Spontaneous Heterotopic Pregnancy: Dual Case Report and Review of Literature. Case Reports in Obstetrics and Gynecology. 2145937.