
World Journal of Radiology and Imaging(WJRI)
ISSN: 2835-2440 | DOI: 10.33140/WJRI


Case Study - (2024) Volume 3, Issue 1
A Rare Case of Entrapment Neuropathy of the Optic Nerve in Optic Canal Stenosis
2Diagnostic Radiology Department, West Hospital, Azerbaijan
3Diagnostic Radiology Department, Mediland Hospital, Azerbaijan
4Diagnostic Radiology Department, Avrasiya Hospital, Azerbaijan
Received Date: Jun 14, 2024 / Accepted Date: Jul 09, 2024 / Published Date: Jul 16, 2024
Copyright: ©Â©2024 Ayaz Kamil Hidayatov, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Bayramov, R. B., Hidayatov, A. K., Ismayilzada, K. I., Huseynova, S. D. (2024). A Rare Case of Entrapment Neuropathy of the Optic Nerve in Optic Canal Stenosis. World J Radiolo Img, 3(1), 01-03.
Abstract
Optic canal stenosis is occasionally associated with osteoplastic diseases such as fibrous dysplasia, osteopetrosis and Paget disease. Nevertheless, hyperostosis and exostosis are also can cause of optic canal narrowing and stenosis. This entity also has been described in familial hypophosphatemic rickets and mucopolysaccharidosis type 4. Idiopathic non-lesional optic canal stenosis has never been reported to induce symptomatic entrapment of the cranial nerve, such as visual disturbance or vision loss. In this report we describe an extremely unusual case of entrapment neuropathy of the optic nerve caused by non- lesional optic canal stenosis. According to the published literature reviewed thus far, this is the first reported case of entrapment neuropathy of the cranial nerve caused by idiopathic narrowing of the optic canal.
Keywords
Optic Canal, Optic Canal Stenosis, Entrapment Neuropathy, Magnetic Resonance Imaging, Computed TomographyIntroduction
The optic canal is a cylindrical canal running through the lesser wing of the sphenoid bone and communicating channel between the orbit and middle cranial fossa, opening into the skull base at the optic foramen. The optic canal forms a passage for the optic nerve, symphatetic fibers, meningeal sheaths and ophthalmic artery. Optic canal is the narrowest part of the optic nerve subarachnoid space. Given the delicate neurovascular structure that passes through the narrow or stenotic optic canal, understanding this canal’s dimensions, anatomical variations, and their relationships is essential for effective diagnostic medicine and surgical management.
While there have been prior studies regarding the narrowing of the optic canal due to osteoplastic diseases and most have focused on lesional canal stenosis. Furthermore, some studies have noted asymmetry of the optic canal in patients with asymmetrical degrees of glaucoma and papilloedema.
We report a case of unilateral optic nerve entrapment in 17-years- old male caused non-lesional optic canal stenosis. Our case includes clinical presentation, computed tomography and magnetic resonance imaging findings.
Case Report
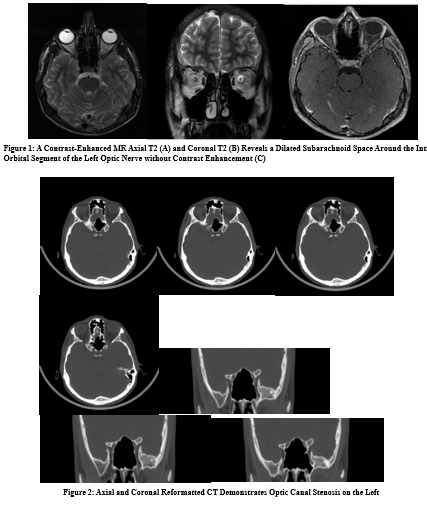
A 17-year-old boy presented with impaired visual acuity and blurred vision in the left eye. His complaints started one year ago. There was no prior history of malignancy, surgery, or trauma. Results of an ophthalmological examination revealed that his left- sided visual acuity had decreased to 0.4 and could not be corrected; visual acuity in his right eye was normal. A fundus examination conducted by an ophthalmologist revealed left-sided optic atrophy in the macula lutea region. The patient underwent to magnetic resonance imaging (MRI) to exclude intracranial pathology. A contrast-enhanced MR reveals a dilated subarachnoid space around the intra-orbital segment of the left optic nerve without contrast enhancement. The cavernous sinuses were normal. There was no focal brain lesion. Computed tomography (CT) was suggested to evaluate of the optic canal and skull base bony structures. CT demonstrates severe narrowing of the left optic canal. The width at the center of the left optic canal was measured at 1.74 mm and 4.06 mm on the right. The length of the optic canal was measured at 1.29 cm and 1.30 cm respectively.
Discussion
The optic nerve, a major component of the visual system, is divided into four segments: the intrabulbar, the intraorbital, the intracanalicular and the intracranial [1]. Radiographic description of optic canal was first described by Winckler in 1901, and its oblique position was observed by Rhese [2]. The optic canal passes through the root of the lesser wing of the sphenoid bone, connecting the middle cranial fossa to the orbit. The length of the optic canal measures approximately 4.5-15 mm. The superior wall of the optic canal is formed by a thin bony lamina separating it from the anterior cranial fossa. The optic canal is bounded laterally and inferiorly by the anterior clinoid process of the lesser wing of the sphenoid bone and contacts the sphenoid sinus and the sphenoethmoidal air cells medially.
We analyzed published results and statistical analysis according to optical canal asymmetry and optic canal stenosis. We found that a significant difference was seen among males, between the left and right sides for width at mid-length of the optic canal. In females, no significant difference was seen between the optic canal’s left and right side sizes [3]. Optic canal shape has been quoted in previous studies as hourglass, cone, or cylindrical shaped and the narrowest point of the optic canal was orbital opening [4,5]. The measurement of the optic canal is extremely important in light of the fact that the optic canal connects the subarachnoid space of the intraorbital part of the optic nerve with the intracranial cerebrospinal fluid space. Recent publications suggest that circulatory dysfunction of cerebrospinal fluid may be a factor responsible for papilledema [6-8].
In the present case, the shape of the bilateral optic canal is cylindrical, and the whole segment of the left optic canal is stenotic. The subarachnoid space around the intraorbital segment of the optic nerve was dilated and there was no contrast enhancement which indicates the entrapment neuropathy and explains patient’s symptoms. We have decided that it is not physiological asymmetry, but narrowing or stenosis of the optic canal.
Conclusion
In conclusion, we present a very rare case of entrapment neuropathy of the optic nerve due to optic canal stenosis. Optic canal stenosis is mostly associated with fibrous dysplasia, osteopetrosis, Paget disease, exostosis, familial hypophosphatemic rickets, and some types of mucopolysaccharidosis.
Conflict of interest
The authors state that there is no conflict of interest.
References
- Radunovic, M., Vukcevic, B., Radojevic, N., Vukcevic, N., Popovic, N., & Vuksanovic-Bozaric, A. (2019). Morphometric characteristics of the optic canal and the optic nerve. Folia Morphologica, 78(1), 39-46.
- Hammerschlag, S. B., O'Reilly, G. V., & Naheedy, M. H. (1981). Computed tomography of the optic canals. AJNR: American Journal of Neuroradiology, 2(6), 593.
- Sthapak, E., Pasricha, N., Narayan, S. et al. Optic canal: a CT- based morphometric study in north Indian population. Egypt J Neurosurg 38, 46 (2023).
- Guseva, Y. A., & Denisov, S. D. (2006). Structure of the optic canal in human ontogenesis. Annals of Anatomy-Anatomischer Anzeiger, 188(2), 103-116.
- Sinanoglu, A., Orhan, K., Kursun, S., Inceoglu, B., & Oztas, B. (2016). Evaluation of optic canal and surrounding structures using cone beam computed tomography: considerations for maxillofacial surgery. Journal of Craniofacial Surgery, 27(5), 1327-1330.
- Killer, H. E., Laeng, H. R., Flammer, J., & Groscurth, P. (2003). Architecture of arachnoid trabeculae, pillars, and septa in the subarachnoid space of the human optic nerve: anatomy and clinical considerations. British Journal of Ophthalmology, 87(6), 777-781.
- Wostyn, P., De Groot, V., Van Dam, D., Audenaert, K., Killer, H. E., & De Deyn, P. P. (2015). Glaucoma and the role of cerebrospinal fluid dynamics. Investigative ophthalmology & visual science, 56(11), 6630-6631.
- Hayreh, S. S. (1964). Pathogenesis of oedema of the optic disc (papilloedema). Br J Ophthalmol, 48, 522-543.