

Research Article - (2022) Volume 6, Issue 2
A Prospective Study on Clinico-Radiological & Pathological Correlation in Musculoskeletal Tuberculosis
2Agarwal Varun Kumar, Assistant Professor, Department of Orthopaedics, Rohilkhand Medical College and, India
3Narula RK., Professor, Department of Orthopaedics, Rohilkhand Medical College and Hospital, Bareilly, India
4Somashekarappa T., Professor and Head, Department of Orthopaedics, Rohilkhand Medical College and Ho, India
Received Date: Sep 30, 2022 / Accepted Date: Oct 02, 2022 / Published Date: Nov 26, 2022
Copyright: ©Ã?©2022 Varun Kumar Agarwal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Singh, G., Agarwal, V.K., Narula, R.K., Somashekarappa, T. (2022). A prospective study on clinico-radiological & pathological correlation in musculoskeletal tuberculosis. Stem Cell Res Int, 6(2),132-139.
Abstract
Background: To analyse how dependable Clinical, Radiological and Pathological features are in establishing a diagnosis of Musculoskeletal Tuberculosis and to identify other pathological conditions mimicking musculoskeletal tuberculosis.
Materials and Methods: The present prospective study include total of 110 patients in the study. All patients were clinical and radiologically examined. Then patient underwent percutaneous biopsy of the involved region and tissue samples were subjected to histopathological examination and CBNAAT for definitive diagnosis of musculoskeletal tuberculosis.
Results: The study includes 110 cases, male preponderance (65.5%) was seen in comparison to females (34.5%). Clinically and radiologically, dorsal spine (35.5%) and lumbar spine (28.2%) were the most common site of involvement. Out of 110 patients, 100 were confirmed as musculoskeletal tuberculosis by histopathology and molecular diagnosis. Histopathology alone could make diagnosis in 92 cases and molecular diagnosis in 100 cases and 10 cases were non-tuberculous in etiology (metastatic deposits of carcinoma in 5 cases, pyogenic spondylodiscitis in 3 cases and primary neoplastic lesion in 2 cases (giant cell tumour and haemangioma).
Conclusion: Musculoskeletal Tuberculosis is a deep seated and paucibacillary condition difficult to diagnose due to inadequate sample. Therefore, multipronged approach by direct smear examination, histopathological examination, molecular diagnosis is required for early diagnosis. Culture is gold standard for diagnosis but can be negative in partially treated cases. CBNAAT is highly sensitive and specific that enables rapid detection of tubercular bacilli but an give false positive results in non-viable bacilli.
Keywords
Musculoskeletal tuberculosis, Percutaneous biopsy, Histopathological examination, CBNAAT
Introduction
Tuberculosis (TB) is an infectious disease caused by Mycobac- terium Tuberculosis. India alone has 1/5 of the total world pop- ulation of tubercular patients [1, 2]. Among 8.6 million people who developed tuberculosis about 3% were estimated to have musculoskeletal tuberculosis in [3]. Of all the patients suffering from tuberculosis, nearly 1-2% have involvement of the skeletal system with spinal tuberculosis being the most common form of skeletal tuberculosis, constituting about 50% of all cases [4].The musculoskeletal TB is difficult to diagnose due to its non-specific symptoms. Imaging plays an important role in early diagnosis of Musculoskeletal tuberculosis. Biopsy of the involved region help in increasing the yield of definitive diagnosis in case of suspected musculoskeletal tuberculosis.
CBNAAT is a fast and accurate alternative diagnostic test to culture in musculoskeletal tuberculosis .It a fast and accurate alternative diagnostic test to culture in musculoskeletal tuberculosis .Culture is the gold standard technique for the diagnosis of musculoskeletal tuberculosis but can be negative in partially treated cases and has slow replication rate of 6–8 week period; and it requires 10– 100 bacilli/mL (live bacilli) in clinical specimens to become culture positive. The objective of study is to analyse how dependable Clin- ical, Radiological and Pathological features are in establishing a diagnosis of musculoskeletal Tuberculosis and to identify other pathological conditions similar to skeletal tuberculosis.
Materials and Methods
The present prospective study was conducted in the Department of Orthopaedic Surgery, Rohilkhand Medical College, Bareilly from November 2017 to November 2018 with the objective to study the Clinico-radiological & Pathological correlation in Musculoskel- etalm Tuberculosis. A total of 110 patients were included in the study.
Inclusion Criteria:
• Patients of all age group.
• Patient willing to give informed consent.
• Patients of both sexes.
• Patient with clinical and / or radiological features suggesting of musculoskeletal tuberculosis.
• Any patient not responding to ATT.
• Any patient who was suspected for any other pathology but biopsy came out to be tuberculosis.
Exclusion Criteria:
• Patient not giving consent.
• Patient not willing for biopsy.
• Any contraindication for biopsy or surgery.
• Biopsy not obtainable (inaccessible sites).
Full history was obtained from each patient, and they were ex- amined clinically. Then following investigations were done Hae- moglobin, TLC, DLC, ESR, CRP, Chest X-ray, X-ray of involved region, MRI of involved region, Biopsy of the involved region for histopathological examination, AFB staining, culture and sensitiv- ity, routine microscopy and other relevant investigations. Clinical diagnosis was made on the basis of signs and symptoms of the patients like –
1. In spinal tuberculosis - Backache is the most common symptom and there may be localized kyphotic deformity with muscle power weakness. Paraspinal muscle spasm, abscesses and sinuses may be present. Constitutional symptoms like malaise, loss of weight, loss of appetite, night sweats and evening rise of temperature.
2. In tuberculosis of hip - Pain, limping, deformity, sinuses, ab- scess and fullness around the hip with and without constitutional symptoms.
3. In tuberculosis of knee joint – pain, swelling around knee joint, boggy synovium, sinuses, deformity, subluxation and constitution- al symptoms.
4. In tubercular osteomyelitis -pain, swelling of bone with warmth and tenderness, overlying boggy swelling of soft tissues, abscess or sinus formation, and enlargement of regional lymph nodes.
Radiological findings in musculoskeletal TB are often non-specific and indicative infective etiology, rather than the causative organ- ism. Initially, X-ray of the involved region and further evaluation with MRI, CT, or ultrasound is done. MRI in spinal tuberculosis suggestive of destruction of endplates with disc space reduction, pre and paravertebral collection, abscesses and localised osteo- porosis and In MRI of tubercular arthritis —synovitis, active and chronic pannus, periarticular inflammation, articular erosions, car- tilage destruction, abscesses, tenosynovitis, bursitis and marrow edema. After clinical and radiological examinations, percutaneous biopsy of the involved region was done and send for CBNAAT and histopathological examination.
Percutaneous biopsy procedure
Transpedicular approach [Figure 1]- The patient is placed in the prone position under local anaesthesia and the needle is intro- duced along the course of the pedicle to penetrate the vertebra at the groove between the transverse process and the lateral aspect of the superior articular facet. In this area the cortex is thin and the biopsy needle is inserted perpendicular thereby decreasing the incidence of slippage. More than 50% of the cancellous bone the vertebral body is accessible through this approach. The potential risk of this procedure is violation of the inferior and medial wall of the pedicle, which may lead to hematoma formation, or infection into the spinal canal, which can give rise to spinal cord compro- mise. Consideration of dimension of the trephine and the pedicle is always mandatory. The needle should always be towards the supe- rior and lateral wall of the pedicle. The needle is placed in caudal to cranial angulation than a traditional vertebroplasty approach in an attempt to access intervertebral disk and endplate

Figure 1: Transpedicle Biopsy
Transforminodiscal Approach- The superior concave surface of the vertebra is the entry point of the needle. The superomedial part of the vertebra is not accessible by this approach. Direct Lateral Approach [Figure 2]- for lumbar spine. Patient is placed in later- al position. Level confirmed under c-arm, local anaesthesia given and needle placed retroperitoneal and trans-psoas. Since the biop- sy trocar and needle are thin peritoneal breach doesn’t occur and Lumbar plexus is not damaged.

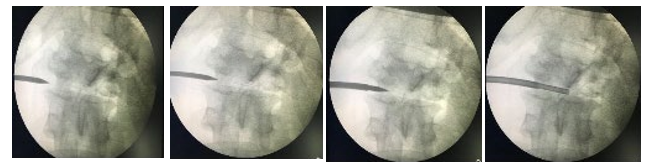
Figure 2: Transdiscal Biopsy through direct lateral approach
Percutaneous Needle biopsy Procedure of knee joint:
Patient is placed in supine position, knee joint painted and drapped, after giving local anaesthesia, a small stab wound about 1 to 2 mm long is made over the medial or lateral aspect of the suprapatellar pouch at the upper level of the patella [Figure 3]. The inner tube is fully inserted into the outer tube, thus covering the opening of the outer tube. The instrument is then directed toward the closest superior angle of the patella. It pierces the synovial membrane and transverses the articular space. At the opposite side of the joint the tip of the outer tube can be palpated through the overlying skin and soft tissues. The inner tube is then withdrawn to open the aperture of the outer tube. That the instrument is in the joint space can be verified by the flow of synovial fluid out of the open end of the tube. Synovial fluid then can be collected for examination. With the inner tube withdrawn at least 1 cm, the hooked tip of the ovoid opening in the instrument is free to catch the synovial membrane. Moderate digital pressure is applied externally on the suprapatel- lar pouch to facilitates the engaging of tissue in the opening. The inner, cutting tube is then fully re-inserted with a rotary movement to cut off the tissue engaged in the opening. The inner tube is again partially withdrawn, and the instrument is then ready to receive an- other specimen from the same area, or it can be moved to another place in the joint space and the same procedure repeated as many times as is desirable or necessary to obtain adequate specimens.
Results
![]() The study includes 110 cases, male preponderance (65.5%) was seen in comparison to females (34.5%). In our study, laborer showed the higher incidence (37.5%) of involvement.
The study includes 110 cases, male preponderance (65.5%) was seen in comparison to females (34.5%). In our study, laborer showed the higher incidence (37.5%) of involvement.
![]() Pain in mid-back was the most common symptom among the patients (35.1%). Pain in low back was the second most common symptom among the patients (27.9%) and pain in hip was the third most common symptom among the patients (11.7%).
Pain in mid-back was the most common symptom among the patients (35.1%). Pain in low back was the second most common symptom among the patients (27.9%) and pain in hip was the third most common symptom among the patients (11.7%).
![]() Evening rise of temperature was among 69.1% patients, weight loss was among 67.3% patients and loss of appetite was among 68.2% patients.
Evening rise of temperature was among 69.1% patients, weight loss was among 67.3% patients and loss of appetite was among 68.2% patients.
![]() Deformity was present among 21.8% patients.
Deformity was present among 21.8% patients.
![]() Involvement of Dorsal spine and Lumbar spine was among 35.5% and 28.2% patients.
Involvement of Dorsal spine and Lumbar spine was among 35.5% and 28.2% patients.
![]() Involvement of Hip joint, Knee joint and Wrist joint were seen in 11.8%, 8.2% and 5.5% patients respectively.
Involvement of Hip joint, Knee joint and Wrist joint were seen in 11.8%, 8.2% and 5.5% patients respectively.
![]() Chronic tubercular granulomatous infection containing lang- hans giant cell formation and epitheloid cell formation histological finding was seen among 83.6% patients [Figure 4].
Chronic tubercular granulomatous infection containing lang- hans giant cell formation and epitheloid cell formation histological finding was seen among 83.6% patients [Figure 4].
![]() Chronic non-specific granulomatous infection histological find- ing was seen in 8.2% patients.
Chronic non-specific granulomatous infection histological find- ing was seen in 8.2% patients.
![]() AFB stain and CBNAAT were positive among 21.8% and 90.9% patients respectively [Figure 5].
AFB stain and CBNAAT were positive among 21.8% and 90.9% patients respectively [Figure 5].
![]() Tubercular spondylodiscitis diagnosis was among more than half of patients (58.1%) followed by tuberculosis of hip joint (11.8%), tuberculosis of knee joint (8.2%) and tuberculosis of wrist joint (5.5%) [Figure 6].
Tubercular spondylodiscitis diagnosis was among more than half of patients (58.1%) followed by tuberculosis of hip joint (11.8%), tuberculosis of knee joint (8.2%) and tuberculosis of wrist joint (5.5%) [Figure 6].
![]() The percentage of non-tuberculous lesion was 9%.
The percentage of non-tuberculous lesion was 9%.




Figure 3: Synovial Biopsy for Supra Patellar Pouch
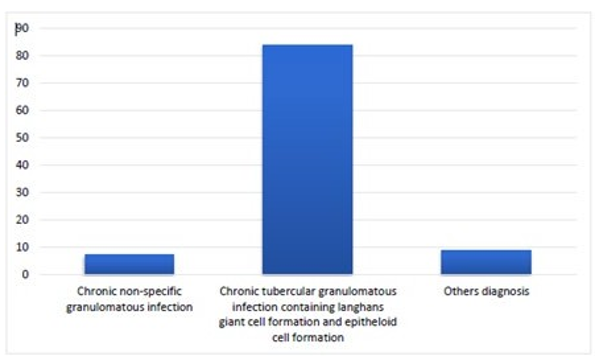
Figure 4: Distribution of patients according to Histological finding

Figure 5: Distribution of patients according to microbiological finding

Figure 6: Distribution of patients according to diagnosis
Discussion
Tuberculosis is the most common infection worldwide and it can affect any part of the body, most commonly lungs. The spine is affected in almost 50% cases of skeletal tuberculosis. Tuberculous of spine causes bony destruction and collapse of the vertebrae, ky- photic deformity, paravertebral abscess, psoas abscess, interver- tebral disc involvement, epidural abscess and edema in the soft tissue planes [5]. In this study, pain in mid-back was the most common presenting symptom among the patients (35.1%). Pain in low back was the second most common symptom among the mon symptom among the patients (11.7%). found that 45 patients (90.4%) presented with pain and difficulty while walking followed by backache in 29 patients (55.8%) and discharge from joints in 25 patients (48.1%) [6].
In the present study, constitutional symptoms like evening rise of temperature was among 69.1% patients and weight loss was among 67.3% patients. Loss of appetite was among 68.2% patients. Found that constitutional symptoms of tuberculosis like fever and weight loss were in 24 (46.2%) and 22 patients (42.3%) respectively [6]. (45%) and (39%) reported almost similar findings in their study. In this study, deformity was present among 21.8% patients. Kyphotic deformity wasm among 45.8% patients and Flexion, adduction, internal rotation and apparent shortening was among 25% patients [7, 8]. Flexion, abduction, external rotation and apparent length- ening was among 20.8% patients. Angular kyphotic deformity and Scoliotic deformity each was present in 4.2%patients.
The radiological findings of this study showed that dorsal spine and Lumbar spine was among 35.5% and 28.2% patients. Hip joint, Knee joint and Wrist joint were seen in 11.8%, 8.2% and 5.5% patients respectively. The other radiological features were less than five % in his study on the epidemiologic parameters of osteoarticular tuberculosis founded that the spine was the most commonly affected (50.77%) followed by hip seen in (19.17%) [7]. In his study on clinic- radiological correlation with histopatho- logical and molecular diagnosis in spinal tuberculosis founded that thoracolumbar region was in 30 cases (42.85%), lumbar region in 20 cases cervical in 15 cases (21.42%) and cervicothoracic in 5 cases (7.14%) [9].
In the present study, AFB stain and CBNAAT were positive among 21.8% and 90.9% patients respectively. In his study on Diagnostic accuracy of GeneXpert MTB/RIF in musculoskeletal tuberculosis evaluated 206 biopsies from 201 patients [10]. The sensitivity and specificity of CBNAAT MTB/RIF was 92.3% (84/91) and 99.1% (114/115), respectively. CBNAAT MTB/RIF detected 8.8% more cases than culture (84/91 (92.3%) v. 76/91 (83.5%), respectively; p=0.069). In the present study, chronic tubercular granulomatous infection containing langhans giant cell formation and epitheloid cell formation histological finding was seen among 83.6% patients. Chronic non-specific granulomatous infection histological finding was seen in 8.2% patients showed that histology was positive for TB in all the cases [11].
Tubercular spondylodiscitis diagnosis was among more than half of patients (58.1%) followed by tuberculosis of hip joint (11.8%), tuberculosis of knee joint (8.2%), tuberculosis of wrist joint (5.5%) and non-tuberculous lesion was (9%) includes me- tastasis(4.5%),pyogenic spondylodiscitis(2.7%) and primary neo- plastic lesion(1.8%). Found that One hundred sixty-six cases were histologically proved as tuberculosis and 74 proved to be non-tu- berculous lesions [12]. Reported that diagnosis was confirmed on histology in 92% of cases. Reported 70 cases out of which 60 cases were confirmed as spinal tuberculosis by histopathology and CB- NAAT [13, 14].
Histopathological examination alone made diagnosis in 59 cases (98.33%) and CBNAAT in all the 60 cases (100%). In our study out of 110 cases, 74 cases were clinically suspected of Musculo- skeletal tuberculosis undergone radiological investigation which revealed 60 cases of Musculoskeletal tuberculosis which were confirmed by biopsy (HPE 58 cases and CBNAAT 60 cases) and 14 cases as non-tuberculosis underwent biopsy which revealed 11 cases of Musculoskeletal tuberculosis ( HPE 10 and CBNAAT 11) and 3 cases of non-tuberculosis. 36 cases out of 110 cases which were suspected non tubercular undergone radiological investiga- tion revealed 24 cases as Musculoskeletal tuberculosis underwent biopsy and 19 were Musculoskeletal tuberculosis and 5 were non tuberculosis and 12 cases which were radiological non tuberculo- sis underwent biopsy which revealed 10 cases as Musculoskeletal tuberculosis and 2 cases as nontuberculosis. Finally, out of 110 total cases, 100 were diagnosed as musculoskeletal tuberculosis and 10 were diagnosed as non-tubercular disease (Figure 7).

Figure 7: Flow diagram of the present study.
Conclusion
Musculoskeletal tubercular lesion and many other non-tubercular lesion may have similar clinical and radiological features. There is high susceptibility to false positive and false negative result in clinico-radiological diagnosis of musculoskeletal tuberculosis. Lesions like secondaries, pyogenic spondylodiscitis, multiple my- eloma, etc. can mimic musculoskeletal tuberculosis and one can- not afford to delay a definite diagnosis. Therefore, biopsy (histo- pathological examination, CBNAAT and culture) in all cases of suspected musculoskeletal tuberculosis is must to get the accurate diagnosis.
Musculoskeletal Tuberculosis is a deep seated and paucibacillary condition difficult to diagnose due to inadequate sample. Therefore for early diagnosis, multipronged approach by direct smear exam- ination, histopathological examination, molecular diagnosis is re- quired. Culture is gold standard for diagnosis but can be negative in partially treated cases. CBNAAT is highly sensitive and specific that enables rapid detection of tubercular bacilli but can give false positive results in non-viable bacilli. Cost effectiveness is of the restraints for widespread use of CBNAAT. Histopathological ex- amination and CBNAAT are complementary to each other but not a substitute for culture.
The findings of this study can act as a bridge between early di- agnosis of musculoskeletal tuberculosis at community or primary health care center and prevention and treatment of deformity at the earliest possible as these health care centers lack facility for clinical specimen collection from deep joints and diagnosis by conventional methods is difficult. The focus must be to improve access to tertiary care hospitals and specialist care for patients with musculoskeletal TB.
References
- Ansari, S., Amanullah, M. F., Ahmad, K., & Rauniyar, R. K. (2013). Pott's spine: diagnostic imaging modalities and tech- nology advancements. North American journal of medical sci- ences, 5(7), 404.
- Agrawal, V., & Patgaonkar, P. R. (2010). Nagariya. Tubercu- losis of spine. J Craniovertebr Junction Spine, 1(2), 74-85.
- World Health Organization. (2016). World malaria report 2015. World Health Organization.
- Konstantinos, A. (2010). Testing for tuberculosis.
- Shanley, D. J. (1995). Tuberculosis of the spine: imaging fea- tures. AJR. American journal of roentgenology, 164(3), 659- 664.
- Singh, V., Phukan, A. C., & Borgohain, B. Musculoskeletal tuberculosis-A diagnostic dilemma: Clinico-bacteriological study among patients attending tertiary heath care centre in North Eastern India.
- Sharma, V., & Anjum, R. (2016). Epidemiological pattern of osteoarticular tuberculosis in a teaching hospital of rural In- dia: a prospective study. Hip, 37, 19-17.
- Sandher, D. S., Al-Jibury, M., Paton, R. W., & Ormerod, L. P. (2007). Bone and joint tuberculosis: cases in Blackburn be- tween 1988 and 2005. The Journal of Bone and Joint Surgery. British volume, 89(10), 1379-1381.
- Kandala, M., Sugnaneswar, P., Vaishnavi, V., Kandala, V., Kishan, V. T., & Kiran, P. (2017). Clinico radiological correla- tion with histopathological and molecular diagnosis in spinal tuberculosis. MedPulse Int J Orthop, 4(1), 1-5.
- Held, M. F., Hoppe, S., Laubscher, M., Mears, S., Dix-Peek,S., Zar, H. J., & Dunn, R. N. (2017). Epidemiology of mus- culoskeletal tuberculosis in an area with high disease preva- lence. Asian Spine Journal, 11(3), 405.
- Jain, A. K., Jena, S. K., Singh, M. P., Dhammi, I. K., Ramach- adran, V. G., & Dev, G. (2008). Evaluation of clinico-radio- logical, bacteriological, serological, molecular and histologi- cal diagnosis of osteoarticular tuberculosis. Indian journal of orthopaedics, 42(2), 173.
- Shaikh, S. I., Chauhan, A. A., & Patel, U. (2013). An analy- sis of clinico-radiological and histopathological correlation in Tuberculosis of spine. National journal of medical research,3(03), 198-202.
- Rafiqi, K., Yousri, B., Arihi, M., Bjitro, C., Aboumaarouf, M., & El Andaloussi, M. (2013). Unusual locations of osteoartic- ular tuberculosis in children: a report of 12 cases. Orthopedics & Traumatology: Surgery & Research , 99 (3), 347-351.