



Research Article - (2023) Volume 8, Issue 3
A Meta-Analysis Study on Internal Compression Therapy (ICT) in Deep Venous Insufficiency Therapy
Received Date: Aug 24, 2023 / Accepted Date: Sep 14, 2023 / Published Date: Sep 19, 2023
Copyright: ©Ã???Ã??Ã?©2023 Rasit Dinc. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Dinc, R. (2023). A Meta-Analysis Study on Internal Compression Therapy (ICT) in Deep Venous Insufficiency Therapy. Cardio Open, 8(3), 66-72.
Abstract
Purpose: To evaluate the effectiveness and safety of the new internal compression therapy (ICT) system in deep vein insufficiency (DVI). Surgical treatments are impractical, and the success rate is lower in the treatment of deep vein insufficiency (DVI). We have developed a new technology called the ICT valve leak sealer reconstruction system (Invamed, Ankara/Turkey) for the treatment of primary DVI by applying internal compression.
Methods: Three research articles evaluated in this meta-analysis study, searched PubMed and Scholar Google using the words "internal compression therapy" and deep vein insufficiency therapy. Original full text articles on the ICT System for the treatment of DVI considered eligible studies published until July 2022.
Results: In the included studies, the procedure time was 11-23 minutes. At the end of one year or more of follow-up, the anatomical success rate was greater than 92%. The diameters of the veins decreased significantly. Venous Clinical Severity Score (VCSS) and Quality of Life (QoL) scores have improved at statistically significant rates.
Conclusion: ICT is a minimally invasive, fast, safe, and effective percutaneous method for the treatment of patients with DVI. The procedure applied in outpatient conditions and improves the patient's clinic in a short time.
Keywords
Internal Compression Therapy (ICT), Deep Vein Insufficiency (DVI), Cyanoacrylate
Introduction
Chronic venous insufficiency (CVI) is a major public health problem, as it affects approximately 30% of the general popula- tion and gradually deteriorates the patient's quality of life [1,2]. While it most commonly affects the superficial veins, it also af- fects the deep veins or perforating veins, and it may occur as combinations of these insufficiencies [3]. Venous insufficiency is seen primarily in the lower extremities, with the incidence of superficial and deep venous insufficiency (DVI) in the lower extremities being 90% and 30%, respectively [4].
In the treatment of CVI, the objective is to eliminate or at least reduce reflux in venous insufficiency, which results in health costs and loss of work force by causing infection, excessive swelling, soft tissue ulceration, and deep vein thrombosis (DVT) [5]. In the treatment of superficial venous insufficiency (SVI), there are different treatment options in addition to conservative and surgical treatments. Endovenous thermal ablations (EVTA) such as endovenous laser ablation (EVLA) and radiofrequency ablation (RFA), and more recently, nonthermal nontumescent (NTNT) applications such as catheter-guided cyanoacrylate ad- hesive closure (CAC) systems and mechanochemical ablation techniques have achieved significant successes in the treatment of SVI [6-10].
However, none of the therapeutic modalities is satisfactory and there is still a large gap in the management of DVI [4]. Medical compression therapies remain the cornerstone of conservative management of DVI due to the less successful outcomes and the impracticality of the surgical treatments [11-17]. In fact, external compression of the leg prevents or reduces blood backflow by reducing the diameter of the vein lumen and improving venous calf pump function [11,18]. This reduction in reflux prevents the occurrence of DVT, post-thrombotic syndrome, and leg ulcers [19-21]. In this regard, different compression modalities contin- ue to be tried as treatment options to improve the condition of patients with lower leg deep vein insufficiency [22,23].
In this context mentioned, we (Invamed RD Global, Ankara, Turkey) have developed a new technology called the ICT Val- vular Leak Sealer Reconstruction System for the treatment of primary DVI by applying internal compression [5,24,25]. In this system, a mixture of hyaluronic acid and hard n-butyl-2-cyano- acrylate (NBCA) gel is administered to the outer surface of the vein using the ICT device at the insufficient valve level between the deep vein and the muscle fascia. The mixture of hyaluronic acid and NBCA adheres around the valves and forms an exoskel- eton with a nonabsorbable biopolymer around the vessel wall. Thus, this device allows the valves to approach each other by reducing the diameter of the vein and increasing their functions. This current meta-analysis study aimed to assess the efficacy and safety of ICT in the treatment of deep vein insufficiency of the lower extremities.
Methods
Study Design and Database Search
This meta-analysis study conducted in accordance with the guidelines provided by Preferred Reporting Items for System- atic Reviews and Meta-analyses (PRISMA) [26]. We searched PubMed and Scholar Google using the words "internal compres- sion therapy" and deep vein insufficiency therapy. Original full text articles on studies using the ICT valve leak sealer recon- struction system for the treatment of DVI considered eligible studies that published until July 2022 (Figure 1).
 \
\
Figure 1: The PRISMA Diagram Regarding to Study Design and Database Searching
Data Assessment
Two independent commentators (N.A., E.A.) evaluated the data. In case of any disagreement, it was resolved by negotiating with the article's author (R.D).
Data Analysis
The mean difference (MD) used as the effect size of the venous clinical severity scores (VCSS) and the mean values of the mea- surement of the vein diameter before and after the procedure, both indicators of treatment success. The meta-analysis of these difference values, fixed effects, random effects subtitled weight coefficients, mean difference, and 95% confidence interval (CI) values were presented in Tables and Figures. To determine whether the studies included in the meta-analysis have publi- cation bias, primarily the funnel plot used and then the Begg and Mazumdar rank correlation statistics were calculated. A for- est chart with 95% CI used to graphically display the estimated weight results from the studies.
The Chi-square heterogeneity test with (k-1) degrees of freedom, known as the Cochrane Q statistic, used to evaluate heterogene- ity. Heterogeneity indicated by I2. According to the heteroge- neity status, the significance evaluated with the fixed effect and random effect model. If the I2 value is less than 25%, it is de- termined as low heterogeneity, 26-75% moderate and over 75% high heterogeneity. The MedCalc statistical package program (MedCalc Software, Ostend, Belgium) used to evaluate the data.
Results
Table 1 shows the distribution of sex and mean age of the pa- tients according to the studies included in the evaluation.
|
Study Name |
Gender (male–female) n (%) |
Age Mean ± Standard Deviation |
|
Yavuz et al. [24] |
172 (60.2%)–114 (39.8%) |
55±13.2 |
|
Eroglu et al. [3] |
12(40 %)-18(60 %) |
40.9 ± 7.6 |
|
Tural et al. [11] |
4(36.4 %)-7(63.6 %) |
54.3±13.7 |
Table 1: Distribution of the Mean Age and Gender of the Patients Included in the Studies
The representations of funnel plots presented in Table-2 and Fig- ures 2A and B, respectively. As seen in Table 2 in the publication bias analysis, it was supported that there was no publication bias since the p values were greater than 0.05.a
|
Parameters |
Kendall’s Tau |
p value |
Interpretation |
|
VCSS |
1.01 |
0.12 |
There is no significant bias (p>0,05) |
|
Vein Diameter |
0.33 |
0.61 |
There is no significant bias (p>0,05) |
*Begg’s test
Table 2: Data Analysis of Publication Bias
When the funnel plot graphs in Figures 2A and B examined, it seen that the majority of the article study included in the re- search is symmetrically distributed. As we see in Table 3, VCSS shows a moderate heterogeneous distribution, and a random ef- fects model recommended for its evaluation. On the other hand, vein diameters show a homogeneous distribution, and a fixed-ef- fects modelrecommended for them.

Figure 2: Funnel Plots Representation of Publication Bias for VCSS and Vein Diameters
|
|
p value |
I2 (%) |
Interpretation |
|
VCSS |
0.12 |
43 |
It shows a moderate heterogeneous distribution, and a random effects model is recom- mended. |
|
Vein Diameter |
0.82 |
0 |
It shows homogeneous distribution, and a fixed effect model is recommended. |
I2 value: <25% low heterogeneity; 26-75% moderate heterogeneity; >75% high heterogeneity
Table 3: Analysis of Heterogeneity
According to the results of the 3 studies included in the study, according to the random effects model, the mean difference of the VCSS values in the pre- and post-procedure periods was 7.3, while these differences ranged from 2.54 to 12.07 (Table-4, Fig- ure 3A). Because of this evaluation, it was evidence-based that there was a difference in mean VCSS values (p<0.01).
|
Study |
Sample size |
MD (95% CI) |
z |
P |
Weight (%) |
|
|
Fixed |
Random |
|||||
|
Yavuz et al. [24] |
286 |
16.8(5.64-27.96) |
|
|
3.68 |
14.09 |
|
Eroglu et al. [3] |
30 |
5(2.65-7.35) |
|
|
83.01 |
53.94 |
|
Tural et al. [11] |
11 |
7(1.13-12.87) |
13.31 |
31.97 |
||
|
Total (fixed effects) |
327 |
5.7(3.56-7.84) |
5.218 |
<0.001 |
100 |
100 |
|
Total (random effects) |
327 |
7.3(2.54-12.07) |
3.003 |
0.003 |
100 |
100 |
MD: mean difference
Table 4: Meta-Analysis of the Mean Difference in VCSS between the Pre-And-Post-Procedure Periods
According to the results of the 3 studies included in the study, according to the fixed effects model, the mean difference of the diameter values of the vein in the pre and post procedure periods was 3.12, while these differences ranged from 1.47 to 4. 76 (Table 5, Figure 3B). Because of this evaluation, it was ev- idence-based that there was a difference in the mean vein diam- eter values (p<0.01).
|
Study |
Sample size |
MD (95% CI) |
z |
P |
Weight (%) |
|
|
Fixed |
Random |
|||||
|
Yavuz et al. [24] |
286 |
3.4(1.78-8.56) |
|
|
10.05 |
10.05 |
|
Eroglu et al. [3] |
30 |
2.78(0.81-4.76) |
|
|
69.17 |
69.17 |
|
Tural et al. [11] |
11 |
4.1(0.49-7.71) |
20.78 |
20.78 |
||
|
Total (fixed effects) |
327 |
3.12(1.47-4.76) |
3.716 |
<0.001 |
100 |
100 |
|
Total (random effects) |
327 |
3.12(1.47-4.76) |
3.716 |
<0.001 |
100 |
100 |
Table 5: Meta-Analysis of the Mean Difference in Vein Diameters between the Pre-And-Post-Procedure Periods
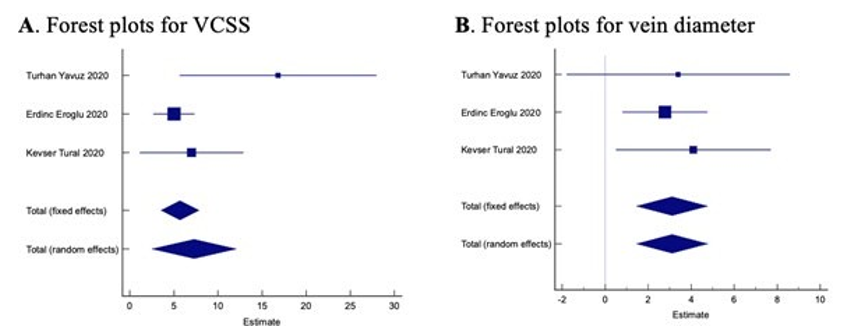
Figure 3: Forest Plot for VCSS and Vein Diameters
Discussion
DVI, a deficiency in the transfer of blood in the deep venous system of the lower extremities to the caval system, may occur as a complication of proximal vascular obstruction or may be present in the primary form due to valve failure or congenital valve malformation [3]. Despite the various techniques applied, mainly surgical, the huge gap in DVI treatment remains a ma- jor challenge. Generally, medical compression therapies have an important role for its management [11,17].
In this context, the ICT (Figure 4) method, the application pro- cedure of which is detailed in the included studies, has some ad- vantages over the traditional surgical treatment of DVI. Conven- tional surgical treatments carry certain risks, such as deep vein thrombosis (DVT), surgical infection, postoperative hospitaliza- tion necessity and cosmetic concerns [13-15]. However, ICT is easy to apply and can be applied in outpatient settings. Patients who underwent ICT can usually return home on the same day. In most cases, no antibiotic or anticoagulant treatment [11]. Fur- thermore, conventional surgical treatments for DVI are carried out primarily to provide ulcer regression in patients with the Clinical-Etiological-Anatomical-Pathophysiological (CEAP) score 5-6. Although ICT can be applied to patients with CEAP score 3-4, which allows earlier intervention [14,24].

Figure 4: Internal Compression Treatment (ICT) Valvular Leak Sealer Reconstruction Device and Delivery System
The effectiveness of the method used in the treatment of DVI is evaluated according to several criteria such as changes be- tween CEAP, VCSS and QoL of patients, reflux times and vein diameters before and after the procedure [6,7,14,17,27]. All patients had preoperative CEAP scores above C3 in the three studies included in the current study. At one year or more of follow-up, the overall success rate of the ICT method applied to 317 patients with DVI was greater than 92%. No significant reported procedure-related morbidity or mortality was observed. The processing time has been reported to be as short as 11-23 minutes. Eroglu et al. also reported that quality of life (QoL) scores improved statistically in the post-procedure period. All three studies reported that reflux improved and valvular coapta- tion resulted in success following the procedure by duplex ultra- sound scanning (DUS).
Although retrospective design of the current studies included in the investigation, the bias analysis supported that there was no publication bias for any of the articles, since the p-values were greater than 0.05 (Table 2). Studies are mostly symmetrically distributed in funnel plot graphs, which is related to bias eval- uation for scientific research (Figure 2). When evaluating the heterogeneity test that informs the proportion of variance in the observed effect, VCSS shows a moderate heterogeneous distri- bution, while vein diameters show a homogeneous distribution (Table 3).
The mean difference between the VCSS values before and after the procedure was observed to be 7.3 and was evidence-based with p<0.01 (Table-4, Figure-3A). The mean difference for vein diameters was 3.12 and was evidence-based with p<0.01 (Ta- ble-5, Figure-3B). These observations strongly encourage the application of ICT in DVI treatments. In this system, the hy- aluronic acid in the mixture strengthens the connective tissue around the vessel, while the cyanoacrylate solidifies with po- lymerization and acts as an exoskeleton [28]. This system helps to restore the venous valve function by reducing the lumen diam- eter of the vein, which allows the valvular re-coaptation. In some experimental studies, the compression effect of ICT application on the vessel has been reported to continue and cyanoacrylate is as durable as sutures [24]. Despite the durability of cyanoacry- late, no serious adverse effects of ICT application were reported during short- or mid-term follow-up, as well as the experimen- tal studies [3,5,11,24,28]. To date, toxicological, carcinogenic, and mutagenic effects against hyaluronic acid and cyanoacrylate have also not been reported in vascular use [24]. The findings indicate that ICT is effective, safe, and even user-friendly.
Unlike other investigators used for DVI, Bolat et al evaluated the efficacy of the ICT method in patients with chronic superfi- cial venous insufficiency [5]. They reported that reflux time and VCSS improved significantly. Great saphenous veins have even been reported to be effectively and safely treated with micro- foam sclerotherapy without postoperative symptoms when the lumen of the vessel is reduced by perivenous injection of hyal- uronan gel injection [29].
In an experimental porcine model, Yasim et al, observed increas- es both perivascular collagen I subtype by immunohistochemi- cal staining and connective tissue growth factor (CTGF) mRNA expressions by genetic analysis [28].
Limitation of the Study
Although the preliminary results of the ICT technique show that it is successful, it has some limitations. Since it is a new meth- od, there are only a few studies on the results of this treatment method. Another limitation is the lack of long-term studies for the same reason.
Concluding Remarks
The ICT shows promise for the treatment of patients with deep vein insufficiency. It is a minimally invasive, fast, safe, and ef- fective percutaneous method. This procedure can be performed in outpatient clinics due to its ease of application and early re- covery time. It improves the patient's clinic in a short time, not only in patients with deep venous insufficiency, but also in pa-tients with superficial venous insufficiency.
Ethics Approval Statement
This manuscript, which is a review article, does not include stud- ies with human or animal participants. Institutional review board approval was therefore not required.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Competing interests
RD is president of Invamed RD Global Company.
Authors Contribution
The concept, design and writing of the research was done by Rasit Dinc. Rasit Dinc read and approved final version of the article.
Acknowledgments
The authors thank Prof. Dr. Nurittin Ardic and Bioengineer Esra Akin for the search and evaluation of the data.
References
- Beebe-Dimmer, J. L., Pfeifer, J. R., Engle, J. S., & Schot- tenfeld, D. (2005). The epidemiology of chronic venous insufficiency and varicose veins. Annals of epidemiology, 15(3), 175-184.
- Dimech, A. P., & Cassar, K. (2020). Efficacy of cyanoac- rylate glue ablation of primary truncal varicose veins com- pared to existing endovenous techniques: a systematic re- view of the literature. The Surgery Journal, 6(02), e77-e86.
- Eroglu, E., & Yasim, A. (2018). A randomised clinical trial comparing N-butyl cyanoacrylate, radiofrequency ablation and endovenous laser ablation for the treatment of superfi- cial venous incompetence: two year follow up results. Euro- pean Journal of Vascular and Endovascular Surgery, 56(4), 553-560.
- EroÄ?lu, E., Yasim, A., Doganer, A., Acipayam, M., Ko- carslan, A., Kabalci, M., & Kara, H. (2021). Internal com- pression therapy, a novel method in the treatment of deep venous insufficiency: 18-month clinical results. Phlebology, 36(6), 432-439.
- Bolat, A., & Gültekin, Y. (2022). Effectiveness of internal compression therapy in primary safen vein failure. Anato- lian Current Medical Journal, 4(1), 19-23.
- O’Flynn, N., Vaughan, M., & Kelley, K. (2014). Diagnosis and management of varicose veins in the legs: NICE guide- line. British Journal of General Practice, 64(623), 314-315.
- Proebstle, T. M., Alm, J., Dimitri, S., Rasmussen, L., White- ley, M., Lawson, J., ... & Davies, A. (2015). The European multicenter cohort study on cyanoacrylate embolization of refluxing great saphenous veins. Journal of Vascular Sur- gery: Venous and Lymphatic Disorders, 3(1), 2-7.
- Whiteley, M. S., Dos Santos, S. J., Lee, C. T., & Li, J. M. (2017). Mechanochemical ablation causes endothelial and medial damage to the vein wall resulting in deeper pene- tration of sclerosant compared with sclerotherapy alone inextrafascial great saphenous vein using an ex vivo model. Journal of Vascular Surgery: Venous and Lymphatic Disor- ders, 5(3), 370-377.
- Parsi, K., Roberts, S., Kang, M., Benson, S., Baker, L., Ber- man, I., ... & Yang, A. (2020). Cyanoacrylate closure for peripheral veins: Consensus document of the Australasian College of Phlebology. Phlebology, 35(3), 153-175.
- Bissacco, D., Stegher, S., Calliari, F. M., & Viani, M. P. (2019). Saphenous vein ablation with a new cyanoacrylate glue device: a systematic review on 1000 cases. Minimally Invasive Therapy & Allied Technologies, 28(1), 6-14.
- Tural, K., Günerhan, Y., & Aydın, S. (2020). The effective- ness of internal compression therapy in deep venous insuf- ficiency. Cardiovascular Surgery and Interventions, 7(3), 136-142.
- Nyamekye, I. K. (2022). European Society for Vascular Surgery (ESVS) 2022 clinical practice guidelines on the management of chronic venous disease of the lower limbs. Journal de Medecine Vasculaire, 47(2), 53-55.
- Maleti, O., & Perrin, M. (2011). Reconstructive surgery for deep vein reflux in the lower limbs: techniques, results and indications. European Journal of Vascular and Endovascular Surgery, 41(6), 837-848.
- Maleti, O., Lugli, M., & Perrin, M. (2017). After superficial ablation for superficial reflux associated with primary deep axial reflux, can variable outcomes be caused by deep ve- nous valve anomalies?. European Journal of Vascular and Endovascular Surgery, 53(2), 229-236.
- Leckie, K. E., & Dalsing, M. C. (2018). Open Surgical Re- construction for Deep Venous Occlusion and Valvular In- competence. Surgical Clinics, 98(2), 373-384.
- Mosti, G., & Partsch, H. (2014). Improvement of venous pumping function by double progressive compression stockings: higher pressure over the calf is more important than a graduated pressure profile. European Journal of Vas- cular and Endovascular Surgery, 47(5), 545-549.
- Rohan, P. Y., Badel, P., Lun, B., Rastel, D., & Avril, S. (2015). Prediction of the biomechanical effects of compres- sion therapy on deep veins using finite element modelling. Annals of biomedical engineering, 43, 314-324.
- Ortega, M. A., Fraile-Martínez, O., García-Montero, C., Álvarez-Mon, M. A., Chaowen, C., Ruiz-Grande, F., ... & Bujan, J. (2021). Understanding chronic venous disease: a critical overview of its pathophysiology and medical man- agement. Journal of clinical medicine, 10(15), 3239.
- Bouman, A. C., & Cate-Hoek, A. T. (2014). Timing and du- ration of compression therapy after deep vein thrombosis. Phlebology, 29(1_suppl), 78-82.
- Cosmi, B., Stanek, A., Kozak, M., Wennberg, P. W., Kolluri, R., Righini, M., ... & Szuba, A. (2022). The post-thrombotic syndrome-prevention and treatment: VAS-European inde- pendent foundation in angiology/vascular medicine position paper. Frontiers in Cardiovascular Medicine, 9, 762443.
- Chaitidis, N., Kokkinidis, D. G., Papadopoulou, Z., Hase- maki, N., Attaran, R., & Bakoyiannis, C. (2022). Manage- ment of Post-Thrombotic Syndrome: A Comprehensive Re- view. Current Pharmaceutical Design, 28(7), 550-559.
- Partsch, B., & Partsch, H. (2016). Neue Aspekte der Kom-pressionstherapie. Wiener Medizinische Wochenschrift, 9(166), 305-311.
- Lattimer, C. R., Kalodiki, E., Azzam, M., & Geroulakos, G. (2016). Haemodynamic performance of low strength below knee graduated elastic compression stockings in health, ve- nous disease, and lymphoedema. European Journal of Vas- cular and Endovascular Surgery, 52(1), 105-112.
- Yavuz, T., Acar, A. N., Yavuz, K., & Ekingen, E. (2020). A retrospective study of deep vein insufficiency treatment device: ICT. Annals of Vascular Diseases, 13(3), 255-260.
- Parlar, H., & Arıkan, A. A. (2022). Internal Perivenous Compression for venous insufficiency at the Saphenofem- oral Junction: Early and Midterm Results and Operative Pain. Phlebology, 37(2), 143-148.
- Welcome to the Preferred Reporting Items for SystematicReviews and Meta-Analyses (PRISMA) website.
- Raetz, J., Wilson, M., & Collins, K. (2019). Varicose veins: diagnosis and treatment. American family physician, 99(11), 682-688.
- Yasim, A., Eroglu, E., Kocarslan, S., Yoldas, A., Acipayam, M., Kocarslan, A., & Daglioglu, K. (2021). A New Meth- od Involving Percutaneous Application in the Treatment of Deep Venous Insufficiency: An Experimental Study With Internal Compression Therapy in a Porcine Model. Vascular and Endovascular Surgery, 55(2), 117-123.
- Ragg, J. C., Despa, O. R., Brüggemann, U., El-Chamali, S., & Stoyanova, K. (2017). Foam sclerotherapy of segments of the saphenous vein with adjuvant hyaluronan compres- sion. Phlebologie, 46(02), 81-86.