
Journal of Veterinary Health Science(JVHS)
ISSN: 2831-3887 | DOI: 10.33140/JVHS
Impact Factor: 0.762

Research Article - (2023) Volume 4, Issue 1
A Four-Year Survey of Error Reports In A Radiotherapy Department
2Master of Medical Radiation Engineering/ Department of Radiation Oncology, Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran
3Master Student of Medical physics/Department of Medical Physics, Faculty of Medical Science, Tarbiat modares University, Tehran, Iran
4Radiation Therapist (RTT)/ Shahid Beheshti University of Medical Sciences, Tehran, Iran
5Assistant Professor of Radiation Oncologist / Department of Radiation Oncology, Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran
6Associate Professor of Radiation Oncologist/ Department of Radiation Oncology, Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran
Received Date: Sep 29, 2022 / Accepted Date: Oct 18, 2022 / Published Date: Jan 07, 2023
Copyright: ©Â©2023 Nafise Hasoomi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Esmati E, Hasoomi N*, Khodadadi A, Andish NM, Ghalehtak R, Kazemian A. (2023). A Four-Year Survey of Error Reports in a Radiotherapy Department. J Vet Heal Sci, 4(1), 01-10.
Abstract
Purpose
Patient safety is a fundamental concept in radiotherapy due to the delivery of large radiation doses in a single frac- tion. Radiotherapy is a highly complex procedure with many steps, which confers a high risk of errors. This study aimed to investigate radiotherapy errors and their effects on patients to provide a framework for increasing our knowledge of radiotherapy, quality of treatment and patient safety.
Materials and Methods
The total number of error reports was 648 during four years of this survey (2017-2020), 51% of which were attributed to near-misses, and the patients were not affected by the errors. Also, 40% of the errors were incident errors, while the rest were non-conformity errors. Meanwhile, the number of treatment courses was 12,755, 32,118, 34,052, and 39,784 throughout the survey during 2017-2020, respectively.
Results
The annual error ratio was 2.2 in 100 treatment courses. Use of a collaborative interprofessional approach led to a decrease in the incident errors by 20% and an increase in near-misses by 24% during the survey (P=.002).
Conclusion
Our outcomes indicated that analyzing radiotherapy errors and their effects on patients can help radiotherapy teams, including radiation oncologists, physicists, and radiation therapists, to provide the best services for the patients; it also improves teamwork and increases the quality of treatment.
Keywords
Radiotherapy Errors, Incident Errors, Near-Miss Errors, Patient Safety
Introduction
Radiotherapy is an essential component of cancer treatment. About 50% of cancer patients require radiotherapy for their treat¬ment [1]. Radiotherapy is a highly complex procedure with many steps, which confers a high risk of errors. Although the application of more novel techniques can reduce errors in radiotherapy, it can also be a new source of errors [2, 3].
Patient safety is a fundamental concept in radiotherapy due to the delivery of large radiation doses in a single fraction. The Patient Safety Organization (PSO) has provided a web-based system for radiation oncology specialists, who contribute to the system by recording near-misses and incident errors; this system has been supported by the American Society for Radiation Oncology (AS¬TRO) website [4]. Since some incident errors have serious adverse effects on the human body, it is important to educate the staff about error reporting to prevent them. In this regard, a book, entitled “Toward Safer Radiotherapy” (TSRT), was published by the Na¬tional Patient Safety Agency in 2008, providing practical recom¬mendations to reduce errors and increase treatment safety [5]. In radiotherapy, we can define different categories of errors, such as random and systematic errors. Random errors can originate from repeated measurements under similar conditions. They are defined as a standard deviation (SD) in statistical considerations, poor measurement processes, deviations in recording a parameter, or incorrect procedures, whereas systematic errors involve missing the target volume [6]. Random errors influence systematic errors, which are caused by slight variations in patient positioning in dif¬ferent sessions.
Systematic and random error types that should be prevented and reduced can affect the side effects of tumor control by 10%; there¬fore, it is important to reduce errors and uncertainties to less than 5% [7]. It should be noted that near misses are discovered imme¬diately before treatment delivery and can lead to incident errors if not detected; this type of error is very important, as it represents the protocols of a radiotherapy Center. In organizations with well-trained staff for recording and reporting radiotherapy incidents, it is essential to understand subsequent errors before any unwanted exposure. This is dependent on the performance of quality control teams and their collaboration with other groups working in radio¬therapy centers. Generally, incident errors may occur during con¬ventional treatments or even modern therapies, such as stereotactic body radiotherapy (SBRT), intensity-modulated radiation therapy (IMRT), and volumetric modulated arc therapy (VMAT).
The most important part of radiation is providing reproducibility of the treatment site using different immobilization devices and positioning techniques. The aim of radiotherapy is to deliver radia-tion only to the tumor area and avoid exposing other at-risk organs to radiation. . Complex and rapid technological advances may be associated with errors. To exemplify, a study indicated that Record and Verify (R&V) systems, were responsible for 23% of errors [3]. In another study, use of new technologies and manual beam modifiers was considered as a source of error [8].
Recent studies indicate there is a significant improvements in the error reports through implementing the incident learning system in radiotherapy departmental structure [9, 10]. Marta Bogusz-Czerniewicz, in his study, indicated that incident errors categorized in threes aspects: including organizational standards, physics and technical standards and clinical standards [11]. Sev¬eral researchers have shown that 35-50% of radiotherapy errors are related to beam modifiers [3, 12, 13]. However, image-guid-ed radiation therapy (IGRT) can correct setup errors in real time for each fraction by using two orthogonal radiography films for matching bony landmarks and a rotational scan for soft tissues, which prevent two types of setup errors, that is, interfraction and intrafraction setup errors [14-16]. In this regard, Matthew et al. de¬veloped a near-miss risk index, which scores events on a scale of 0 to 4 (none, mild, moderate, severe, and critical) [17]. The analysis of 2056 incident errors over five years revealed that only 1.95% of them had an impact on the patients, which indicates a substantial decline in the rate of actual and major incidents [18].
Overall, the investigation of errors helps radiotherapy departments to pay more attention to potential errors and avoid systematic and random ones; besides, it can provide different quality assurance protocols [12]. Bogusz-Czerniewicz noted that clear mechanism to monitor and address failure are valuable if they will be imple¬mented, reviewed, audited and improved in place [11].
Incident learning systems can help different organizations to in¬crease patient safety and decrease serious adverse events over time [18-21]. While the majority of radiotherapy error reports are based on reproducibility and setup variations [3, 13, 22-26]. In the pres¬ent study, we aimed to analyze different types of errors in differ¬ent stages of radiotherapy, including computed tomographic (CT) simulation, planning, and treatment, and to introduce methods that can reduce them.
Methods And Materials
This study was conducted in a teaching radiation oncology depart¬ment affiliated to Tehran University of Medical Sciences with four types of conventional and modern linear accelerators. The duration of this survey was four years (2017, 2018, 2019, and 2020). Our radiotherapy center performs two-dimensional (2D) convention¬al radiotherapy, three-dimensional (3D) conformal radiotherapy (CRT), and IMRT techniques, based on the individualized proto¬col (flowchart 1). In our center, 2D conventional radiation therapy accounts for less than 10% of all treatments since 2015, and most techniques are based on 3D CRT and recently IMRT. In our radio¬therapy department, 30 radiation therapists, 10 radiation oncolo¬gists, and 15 physicists, treat 200 patients on a daily basis, using 4 conventional and modern accelerators, including Elekta Compa-ny (Compact & Synergy), and Varian Company (C linac 2100C). Two-thousand patients are treated, and 29,237 treatment courses were delivered annually in this center on average.
Patients, treated exclusively by brachytherapy, were excluded from our analysis. At least 15 parameters (e.g., field dimensions, gantry, couch, and collimator angles, MU, and wedges and etc.) were used for each field. Overall, Elekta accelerators (6-10 MV) treated 43% of selected patients for radiotherapy who suffer from breast cancer and 11% of selected patients for radiotherapy who suffer from head and neck cancer. In addition, 5% of them strug¬gled with mediastinal tumors, 14% with pelvic tumors, and 5% with abdominal tumors were treated using the 18-MV Varian or Synergy accelerator. A special paper-based error report [27] was modified and introduced to volunteer radiotherapy team members, mainly radiation therapists (RTT). This is because RTTs are the last line of treatment procedures and they have the ability to detect errors before the first session of treatment based on the quality control checklist, which is attached to treatment document (Near miss errors), and also they have the responsibility to report their in¬cident errors during the treatment fractions. In our center radiation therapist are responsible for CT Simulation and treatment delivery. They also are responsible for quality assurance of the geometry parameters verification in the document file. Every document of each patients will be verified by a QA member (radiation therapist) in the aspect of the conformity of tumor pathology with the treat-ment area and geometry of plan and recording parameters on the document. To provide a certain protocol for QA, different potential errors were defined in this checklist, which will be mainly checked by radiation therapist. This checklist depicts important factors of the radiotherapy procedures in our oncology department, includ¬ing visits by radiation oncologists, treatment indications, CT sim- ulation or simulation based on the treatment technique, treatment planning, and treatment delivery (Flowchart 1).
Any event, whether it affected the patients or not, was recorded and confirmed for addressing the system shortcomings. Different causes of errors, including external shielding and wedges as sep¬arate sources of errors associated with manual placement, pathol¬ogy, geometric parameters, and setup variations, were analyzed. Each incident recorded in a paper separately. Treatment sites, in¬cluding the head, neck, breasts, pelvis, and extremities, were also investigated in this survey.
In this study, errors were analyzed using four classifications. The first classification divided errors into random and systematic, while in the second categorization, the errors were analyzed at five levels (level 1-3: incident errors; level 4: near-misses; and level 5: non-conformity errors), according to the TSRT book (Figure 4) [5]. In the third categorization, errors were divided based on the cause (Table 1). In the fourth categorization, the percentage of treatment area associated with recording errors indicate 43 % of the patients are breast cancers which covers 23% of error re-ports(Figure 5 & Figure 6). Finally, the root causes of errors were analyzed using the fishbone diagram procedure (Figure 7). The collected data were analyzed using Statistical Package for the So¬cial Sciences (SPSS) for Windows Version 16 (SPSS Inc; Chicago, IL, USA). In all analytical tests, P <0.05 was considered as statis¬tically significant. We used Chi-Square test of independence to de-termine if there is a significant relationship between two nominal (categorical) variables and ANOVA test for significant relationship of continuous variables.
Table 1: Incident Records in Different Years of the Survey Based On the Root Causes
|
ERRORS |
First Year |
Second Year |
third Year |
Forth Year |
|
Pathology and treatment Area |
6 |
4 |
10 |
1 |
|
Incorrect Geometry Parameters& BEV) |
29 |
26 |
38 |
57 |
|
total dose, dose/fraction |
30 |
25 |
20 |
28 |
|
Address |
17 |
6 |
15 |
10 |
|
Radiosensitizer |
3 |
2 |
3 |
0 |
|
Bolus |
21 |
15 |
7 |
7 |
|
Set Up |
22 |
20 |
37 |
15 |
|
Shield design |
1 |
3 |
13 |
3 |
|
Attenuation Factor( Couch & Shield) |
15 |
6 |
5 |
8 |
|
Treatment Planning |
11 |
6 |
7 |
8 |
|
Immobilization & Fixation |
2 |
4 |
6 |
2 |
|
Tattoo |
3 |
2 |
0 |
3 |
|
others |
5 |
0 |
8 |
5 |
Results
The total number of error reports was 648 during four years of this survey, 51% of which were near misses, 40% were incident errors, and the rest were non-conformity errors throughout the survey. For instance, in the third year of the survey, 170 error reports (49% incident errors, 44% near misses, and 7% non-conformity errors) were documented, and error ratio (the number of error reports per new patient) was 10%.
Figure 1 indicates graph of error ratio in the 4 years. In the first, second, third and fourth years of the survey, a total of 162, 116, 170 and 200 error reports per 2185, and 1467, 1555 and 1724 new pa- tients were recorded. Meanwhile, the number of treatment courses was 12,755, 32,118, 34,052, and 39,784, respectively. The analysis of data indicated a statistically significant difference (P<.001) in the increased rate of errors during the survey. As shown in Table 1, the number of reports has been somewhat stabilized, and we have made progress by reducing some of the error causes during the survey, such as treatment planning, attenuation factor calculation, bolus calculation, dose/fraction, setup design, and shield design by 3%(P=.001), 7%(P<.001), 14% (P<.001), 2% P=(.001), 7% (P=.007), and 10%(P<.001) respectively, while other causes, such as geometric parameters, increased by 28%(P<..001).

Figure 1: Error Ratio: Error Report Rates in Different Years of Survey
Table 2: Error Causes Types
|
Geometry parameter Errors |
Treatment Planning Errors |
Set up Errors |
|
wedge angle |
OAR in the treatment field |
overlapping of fields |
|
Shielding |
Isocenter Depth |
geometry parameters (, gantry collimator, MU) |
|
Asymmetric and Symmetric fields |
Overlapping of adjacent fields |
incorrect addressing |
|
Gantry, Couch, collimator angle |
unwanted gap between fields |
treatment extra fraction |
|
SSD |
improper inferior border of breast field |
SSD, Isocenter, VRT |
|
MU |
Addressing |
incorrect Isocenter |
|
Bolus |
CT of contralateral breast |
treatment of thorax instead of Lumbar |
|
couch Factor |
addressing from far marker |
bolus |
|
Attenuation factor of Perspex and Couch |
Medication such as Xeloda |
positioning |
|
incorrect treatment phase |
laser shifting |
thermoplastic shrinkage /contraction |
Figure 2 represent categorical variables of error level in the survey. The most significant number of error reports relates to level 4. As figure 2 illustrates level 4 errors increased significantly in the year 2020. level 1 errors had the lowest frequency which refer to the in-cident errors that means the dose delivered to the patient was more than 20% of the prescribed dose (Figure 2). For example, an organ of a metastatic patient was treated incorrectly for eight fractions. According to Figure 3, the number of incident errors was 72, 49, 84, and 52 respectively during 2017-2020. Also, 88, 61, 75, and 112 near-misses were recorded from 2017 to 2020, respectively.

Figure 2: Frequency of errors in leveling: Frequency of errors based on the 5 levels described in the book Toward Safer Radiotherapy
Some errors were associated with infrastructure factors, and procedures for the final treatment delivery were sometimes un-checked or unverified. Overall, 78.24% of errors were systematic, and 21.76% were random. The most common error category was errors in recording geometric parameters (150 reports) followed by setup discrepancies (94 reports),. More details are presented in Table 1. Figure 2 illustrates the frequency of errors based on the error level(1-5) during 2017-2020. It can be seen that level 4 errors (near-misses) had a higher rates among other levels. Figure 3 rep¬resents the comparison results of incident errors and near misses. Overall, The near-miss errors increased throughout the survey by 24%. In contrast to incident errors that decreased during the sur¬vey by 20% (P=.002).

Figure 3: Comparison of Incident error and near Miss Comparison of Incident Error and Near Miss in Different Years of the Survey
As Figure 4 illustrates, the error frequencies can be categorized based on the organs. Head and neck treatment area had the highest share of reports (35%), followed by breast cancer reports(23%). Moreover, percentage of patients that radiotherapy were an indica¬tion of their treatment are shown in the figure 5.
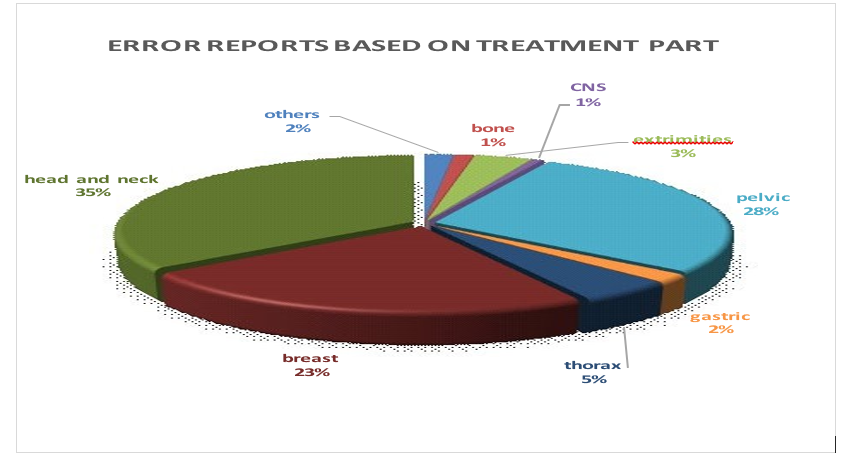
Figure 4: Error Reports Percentages Based On the Treatment Part
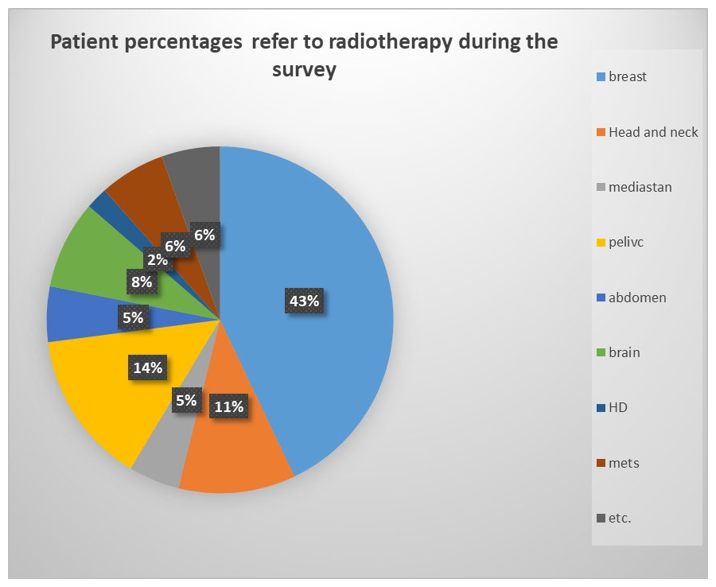
Figure 5: Percentages of Patients Who Suffer From Different Tumors Refer To Radiotherapy in Our Center
In our study, a noteworthy point is that there is a relation between error causes and frequency of different cancers throughout the survey. For example, 49% of patients candidates for radiothera¬py treatment suffer from breast cancer, skin malignancies or some type of sarcoma need bolus in their treatment procedures, while 7.7 % of reports were subjected to bolus errors, therefore, the rate of this error is comparatively low(15%). In contrast, 11% of patients candidate for radiotherapy treatment were head and neck, while the total error rate is almost 35%.
Discussion and Conclusion
Incident learning systems, as a strategy for reporting, analyzing, and presenting methods to prevent errors, have played an essential role in different fields, including airline accidents and nuclear pow¬er [28, 29]. Evidence suggests that comprehensive screening and error recording and reporting can help reduce random and system¬atic errors. Almost 78% of errors in this study were systematic and could be avoided using standard flowcharts and precise screening before the treatment procedure or applying R&V systems.
Error reports of head and neck cancer (35%) indicate that we must be more cautious about this type of cancer (Figure 5 & Figure 6). Our center has employed several methods, such as implementa¬tion of new technologies and several new treatment techniques to make treatment planning as simple as possible. Besides, monitor¬ing methods (using different planning parameters) and different parallel actions were performed to guarantee the treatment pro¬cedure and address the system weaknesses. One of the strategies developed by our multidisciplinary team to address some human errors was the simultaneous checking of the vertical number and source-skin distance (SSD) and verifying that the Beam's eye view (BEV) provided adequate information for radiation therapists to ensure the correct site of treatment. Although R&V systems can reduce many incidents errors, many linear accelerators (LINAC) are still in service, without utilizing R&V systems. A review of the most important finding in our study support Heinrich Accident Triangle theory and Reasons’ Swiss cheese model that near misses and incident errors have similar fundamental causes. The present study offer clear evidence that reduction of near misses will lead to the reduction of incident errors. Overall, error incidents cannot be prevented in the medical environment, but they can be reduced by creating a non-punitive environment that can lead to the detection and correction of medical errors [30, 31].
Errors can be analyzed based on the fishbone diagram or “five-why” flowchart (Figure 6). In this regard, Gregory A et al. reported a fishbone structure and identified different types of errors in ra¬diotherapy, most of which could be prevented [2]. Clearly, incident learning systems in radiotherapy departments can help identify the root causes of errors and increase the knowledge of quality assur¬ance teams and staff [17].
In order to screening the treatment procedure before any expo-sure, level 1 of error occurs at a low frequency in major clinical practices. The role of the quality control team is important in all error levels. In addition, the quality control team can prevent most geometric errors, which may convert to level-3 errors.
Smith showed that the error rate declined over time by 1.3 per 1000 treatment attendances. Our finding imply that the mean annual er¬ror ratio was 2.2 in 100 treatment courses, but the error rates had been increased throughout the survey. One possible conclusion is that in some months, the load of patients and new apprentices in the educational department could lead to more recording errors, which indicates the necessity of more strict regulations in periods of higher clinical load and internship [32].
Wright discovered event reporting had been increased in four dif¬ferent sites. Our study carried out in one center and in 4 years, which indicated an increase in event reporting. It could be related to the dedicating cash award for every event reporting [9].
Implication of the study showed that setup errors also are very important; one reason could be that these type of errors attributed to miss the target volume. Therefore, these findings lead us to be¬lieve that load of patients and the accelerator capabilities are quite important.
Possible explanation for error roots categorization in fish bone di¬agram (figure 6) mean that which team should be responsible to manage and prevent potential errors. Systematic errors were pri¬marily caused when the procedure fails to follow standard proto¬cols, as shown by other researchers [33]. Therefore, most errors can be prevented by adhering to protocols and using flowcharts. Generally, the causes of radiotherapy errors are complex, and it is not ethical to consider only one team to be responsible for them.

Figure 6: Fish Bone Diagram Analysis of Error Roots via Fishbone Diagram
The Safety in Radiation Oncology (SAFRON) and the Radiation Oncology Safety Information System (ROSIS) are two voluntary web-based radiation oncology incident learning systems, devel-oped by the International Atomic Energy Agency (IAEA) and the European Society for Therapeutic Radiology and Oncology (ES-TRO), based on the idea that safety is no accident [34, 35]. In 2011, the ASTRO and the American Association of Physicists in Medicine (AAPM), in collaboration with the Clarity PSO, pro-vided a nationwide incident learning system, called the Radiation Oncology-Incident Learning System (RO-ILS), to share learning experiences with different radiation oncology institutions [36].
Generally, the outcomes of incident learning systems include a sig-nificant shift in the attitude of Radiation Therapists (RTTs). This research provide evidence that we have substantial agreement on system improvement by engagement in individual reporting , safe-ty improvement, concerns about punitive actions, and increased confidence that reporting leads to [17]. A survey indicated that a punitive system and strict rules often do not prevent errors and cannot provide pragmatic solutions [37].
In conclusion, although the rate of radiotherapy errors has not changed over time, an active safety culture and voluntary report-ing have been promoted by the applied methods. Overall, support by the department authorities can provide opportunities to analyze and address errors and increase the quality of treatments using a collaborative interprofessional approach.
Declarations
Funding
There is no funding
Conflicts of Interest/Competing Interests
There is no conflict of interests
Ethics Approval
Not applicable
Consent to Participate
Not applicable Consent for Publication The participants have consented to the submission of this report to the journal
Availability of Data and Material
Derived data supporting the findings of this study are available from the corresponding author on request
Code Availability
Not applicable
Authors' Contributions
Dr. Esmati and Mrs. Hasoomi conceived of the presented idea. Mrs.Hasoomi developed the theory and performed the computa¬tions. Dr Ghalehtaki. And Dr. Esmati verified the analytical meth¬ods. Mrs Khodadadi encouraged Mrs Hasoomi to investigate this comparison between different years and helped Mrs Hasoomi to accumulate data of this work. Mrs Hasoomi performed the anal¬ysis, wrote the manuscript in consultation with Dr Esmati. Mrs Maalandish assist in analyzing data in SPSS. Dr Kazemian pro¬vided critical feedback and helped shape the research. All authors discussed the results and contributed to the final manuscript.
References
- Delaney, G., Jacob, S., Featherstone, C., & Barton, M. (2005). The role of radiotherapy in cancer treatment: estimating optimal utilization from a review of evidenceâ?based clinical guidelines. Cancer: Interdisciplinary International Journal of the American Cancer Society, 104(6), 1129-1137.
- Patton, G. A., Gaffney, D. K., & Moeller, J. H. (2003). Facilitation of radiotherapeutic error by computerized record and verify systems. International Journal of Radiation Oncology* Biology* Physics, 56(1), 50-57.
- Macklis, R. M., Meier, T., & Weinhous, M. S. (1998). Error rates in clinical radiotherapy. Journal of Clinical Oncology, 16(2), 551-556.
- https://www.astro.org/Patient-Care-and-Research/Pa-tient-Safety/RO-ILS.
- Robson, W., Clark, D., & White, N. (2014). Patient safety: the journey towards safer radiotherapy. Journal of Radiotherapy in Practice, 13(2), 129-130.
- Dutreix, A. (1984). When and how can we improve precision in radiotherapy?. Radiotherapy and Oncology, 2(4), 275-292.
- Barthelemy-Brichant, N., Sabatier, J., Dewé, W., Albert, A., & Deneufbourg, J. M. (1999). Evaluation of frequency and type of errors detected by a computerized record and verify system during radiation treatment. Radiotherapy and Oncology, 53(2), 149-154.
- Huang, G., Medlam, G., Lee, J., Billingsley, S., Bissonnette,J. P., Ringash, J., ... & Hodgson, D. C. (2005). Error in the delivery of radiation therapy: results of a quality assurance review. International Journal of Radiation Oncology* Biology* Physics, 61(5), 1590-1595.
- Wright, J. L., Parekh, A., Rhieu, B. H., Miller, D., Opris, V., Souranis, A., ... & Terezakis, S. A. (2019). Adoption of an incident learning system in a regionally expanding academic radiation oncology department. Reports of Practical Oncology and Radiotherapy, 24(4), 338-343.
- Radicchi, L. A., Toledo, J. C., & Alliprandini, D. H. (2020). Critical success factors for implementation of an incident learning system in radiation oncology department. Reports of Practical Oncology and Radiotherapy, 25(6), 994-1000.
- Bogusz-Czerniewicz, M., & Kaźmierczak, D. (2012). Organizational, technical, physical and clinical quality standards for radiotherapy. Reports of practical oncology and radiotherapy, 17(4), 190-199.
- Thwaites, D. (1995). Quality assurance in radiotherapy (ES-TRO advisory report to the Commission of the European Union for the Europe against cancer programme, Grant agreement Soc 95202083). Radiother Oncol. 35: p. 61-73.
- Leunens, G., Verstraete, J., Van den Bogaert, W., Van Dam, J., Dutreix, A., & Van der Schueren, E. (1992). Human errors in data transfer during the preparation and delivery of radiation treatment affecting the final result:“garbage in, garbage out”. Radiotherapy and Oncology, 23(4), 217-222.
- Dawson, L. A., & Jaffray, D. A. (2007). Advances in image-guided radiation therapy. Journal of clinical oncology, 25(8), 938-946.
- Bujold, A., Craig, T., Jaffray, D., & Dawson, L. A. (2012, January). Image-guided radiotherapy: has it influenced patient outcomes?. In Seminars in radiation oncology (Vol. 22, No. 1, pp. 50-61). WB Saunders.
- Guckenberger, M., Meyer, J., Wilbert, J., Baier, K., Mueller,G., Wulf, J., & Flentje, M. (2006). Cone-beam CT based image-guidance for extracranial stereotactic radiotherapy of in-trapulmonary tumors. Acta oncologica, 45(7), 897-906.
- Nyflot, M. J., Zeng, J., Kusano, A. S., Novak, A., Mullen, T.D., Gao, W., ... & Ford, E. C. (2015). Metrics of success: Measuring impact of a departmental near-miss incident learning system. Practical radiation oncology, 5(5), e409-e416.
- Clark, B. G., Brown, R. J., Ploquin, J., & Dunscombe, P. (2013). Patient safety improvements in radiation treatment through 5 years of incident learning. Practical radiation oncology, 3(3), 157-163.
- Arnold, A., Delaney, G. P., Cassapi, L., & Barton, M. (2010). The use of categorized time-trend reporting of radiation oncology incidents: a proactive analytical approach to improving quality and safety over time. International Journal of Radiation Oncology* Biology* Physics, 78(5), 1548-1554.
- Bissonnette, J. P., & Medlam, G. (2010). Trend analysis of radiation therapy incidents over seven years. Radiotherapy and Oncology, 96(1), 139-144.
- Kusano, A. S., Nyflot, M. J., Zeng, J., Sponseller, P. A., Er-moian, R., Jordan, L., & Ford, E. C. (2015). Measurable improvement in patient safety culture: A departmental experience with incident learning. Practical radiation oncology, 5(3), e229-e237.
- Cohen, L., Schultheiss, T. E., & Kennaugh, R. C. (1995). A radiation overdose incident: initial data. International journal of radiation oncology, biology, physics, 33(1), 217-224.
- Ostrom, L. T., Rathbun, P., Cumberlin, R., Horton, J., Gastorf, R., & Leahy, T. J. (1996). Lessons learned from investigations of therapy misadministration events. International Journal of Radiation Oncology* Biology* Physics, 34(1), 227-234.
- Blanco, S., Lopez-Bote, M. A., & Desco, M. (1987). Quality assurance in radiation therapy: Systematic evaluation of errors during the treatment execution. Radiotherapy and Oncology, 8(3), 253-261.
- Swann-D'Emilia, B., Chu, J. C., & Daywalt, J. (1990). Misadministration of prescribed radiation dose. Medical dosimetry, 15(4), 185-191.
- Valli, M. C., Prina, M., Bossi, A., Cazzaniga, L. F., Cosentino, D., Scandolaro, L., ... & Cappelletti, P. (1994). Evaluation of most frequent errors in daily compilation and use of a radiation treatment chart. Radiotherapy and Oncology, 32(1), 87-89.
- Asnaashari, K., GHOLAMI, S., & Khosravi, H. R. (2014). Lessons learnt from errors in radiotherapy centers.
- Johnson, J. L., & Evans, S. B. (2016). The Impact of Incidents: Reporting, Investigating, and Improving. Quality and Safety in Radiation Oncology: Implementing Tools and Best Practices for Patients, Providers, and Payers.
- Ford, E. C., de Los Santos, L. F., Pawlicki, T., Sutlief, S., & Dunscombe, P. (2013). The structure of incident learning systems for radiation oncology. International Journal of Radiation Oncology, Biology, Physics, 86(1), 11-12.
- Heinrich, H. W. (1941). Industrial Accident Prevention. A Sci-entific Approach. Industrial Accident Prevention. A Scientific Approach., (Second Edition).
- Reason, J. (2000). Human error: models and management. Bmj, 320(7237), 768-770.
- Smith, S., Wallis, A., King, O., Moretti, D., Vial, P., Shafiq, J.,... & Delaney, G. P. (2020). Quality management in radiation therapy: A 15 year review of incident reporting in two integrated cancer centres. Technical innovations & patient support in radiation oncology, 14, 15-20.
- Yeung, T. K., Bortolotto, K., Cosby, S., Hoar, M., & Lederer,E. (2005). Quality assurance in radiotherapy: evaluation of errors and incidents recorded over a 10 year period. Radiother-apy and oncology, 74(3), 283-291.
- Radiation Oncology Safety Management system.
- International Atomic Agency. Safety in Radiation Oncology (SAFRON).
- https://www.claritygrp.com/patient-safety-organization/pa-tient-safety-learnings.
- Manning, C. (2007). Dekker S. The Field Guide to Understanding Human Error. Aviation, Space, and Environmental Medicine, 78(2), 148-148.