

Research Article - (2022) Volume 6, Issue 2
A Cross Sectional Study to Evaluate Medication Compliance among Patients with Hypertension
2University of Peloponnese, Department of Nursing, Tripoli, Greece
Received Date: Oct 15, 2022 / Accepted Date: Oct 29, 2022 / Published Date: Nov 02, 2022
Copyright: ©Â©2022 Paraskevi Theofilou. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Theofilou, P., Florou, K., Tsironi, M. (2022). A cross sectional study to evaluate medication compliance among patients with hypertension. Stem Cell Res Int, 6(2),114-120.
Abstract
The purpose of this study is to investigate the level of compliance of patients with hypertension to the medication given to them. For this purpose, a quantitative cross-sectional study was carried out in a sample of 73 elderly patients with hypertension. The Self-Efficacy For Appropriate Medication Use Scale (SEAMS) was used to assess medication com- pliance. The research findings showed that elderly patients with hypertension show a moderate level of compliance to medication. Years since diagnosis, age and years since initiation of treatment were significantly associated with the level of medication compliance in these patients. More studies are needed to illuminate the factors that influence the level of compliance with medication in elderly patients with hypertension.
Keywords
Medication, Compliance, HypertensionA Cross Sectional Study to Evaluate Medication Compliance among Patients with Hypertension
Introduction
High blood pressure (hypertension) is considered one of the most critical public health problems worldwide and is cited as the lead- ing risk factor for both cardiovascular death and hospitalization. Hypertension affects more than 1.5 billion people worldwide and by 2025 approximately 2 billion people will suffer from it [1]. One study showed that the main cause of the global burden of disease was hypertension, which in 2010 accounted for 7% of disabili- ty-adjusted life years (DALYs) and contributed to approximately 9.4 million deaths worldwide annually [2].
Hypertension is a disease of the cardiovascular system and is an important modifiable risk factor for coronary heart disease, heart failure, stroke, kidney failure, kidney dysfunction and eye prob- lems [3]. Hypertension is linked to 70% of strokes and 60.5% of kidney disease and increases the risk of vascular dementia. There- fore, once hypertension is identified, patients should be moni- tored for their blood pressure at regular intervals in order to know whether the blood pressure is adequately controlled or not and take the necessary measures [4].
Although the prevention and control of hypertension has been reported as an important public health issue, finding a strategy to control high blood pressure is a global problem. Several sur- veys from many countries around the world indicated that public awareness of blood pressure levels was poor [5]. Although there are many treatments for hypertensive control, it was reported that even in developed countries such as the United States of Ameri- ca, only one-third of hypertensive patients had controlled blood pressure. It is widely accepted that one of the many factors in the inability to maintain normal blood pressure is the patient's lack of self-management knowledge regarding adherence to pharmaco- logical treatments (such as antihypertensives) and lifestyle modifi- cation (such as diet control, exercise). Poor blood pressure control is the biggest cause increasing the morbidity and mortality of peo- ple with hypertension [3].
Despite significant progress in the diagnosis and treatment of ar- terial hypertension, this condition continues to represent a seri- ous medical, social and economic burden. Blood pressure control, the primary goal of antihypertensive therapy, cannot be achieved even with the most effective drugs without the patient's coopera- tion. However, available evidence suggests that even up to 90% of hypertensive patients may not adhere to their treatments, and approximately 50% of them may discontinue treatment within one year of diagnosis [6].
Compliance with medication is a dynamic process that involves using the medication or a treatment at the prescribed frequency and dose [7]. The effectiveness of drug treatment in hypertensive patients implies the regular correct use of drugs by the patient, combined with compliance with a suitable diet and the adoption of other lifestyle changes. Positive lifestyle changes and compliance with medication significantly reduce complications in hyperten- sive patients [1]. In elderly patients with hypertension, antihyper- tensive therapy is recommended to be applied with caution and prudence due to atherosclerotic changes leading to myocardial ischemia and stroke. Too rapid reduction of blood pressure can contribute to the reduced functionality of vital organs and even worsen ischemic changes [8].
The condition for achieving the desired therapeutic effects is to take drugs according to the instructions and to observe medical recommendations, as well as cooperation at each stage of treat- ment. Unfortunately, lack of cooperation and compliance with an effective treatment regimen is one of the most challenging factors contributing to low treatment success in many chronic diseases [9]. Many factors can affect medication compliance in patients with hypertension. Among these are older age, low level of educa- tion, the possibility of side effects during pharmacotherapy, prob- lems with memory or poor cognition, low socioeconomic status (unaffordable medicine) and lack of adequate information about the use of medicines by health professionals [10].
Some previous studies showed that medication compliance in hy- pertensive patients increases with age [11-13]. However, compli- ance with antihypertensive therapy is not a simple function of age, but may also be shaped by a range of patient-related characteris- tics, such as functional limitations and cognitive impairment [14]. Indeed, some studies have shown an inverse association between age and medication compliance [15, 16]. Thus, a question arises as to whether the elderly, whose mental and physical performance are often impaired demonstrate a high level of medication compliance [14]. The purpose of this study is to investigate the level of com- pliance of elderly patients with hypertension with the medication given to them. In addition, the aim of the thesis was to highlight factors that influence the level of compliance with medication.
Methods
Research design
This is a quantitative cross-sectional study including independent and dependent variables. The dependent variable is the level of compliance among patients while the independent variables in- clude sociodemographic and clinical factors.
Sample
The population of the present study was defined as all elderly pa- tients (over 60 years) with hypertension in Greece. For this pur- pose, a convenience sample was used using the convenience sam- pling method. A total of 100 elderly patients with hypertension were selected to participate in the research, of which 73 finally completed the questionnaire. The criteria for entering the research were: (1) the age of the participants to be over 60 years old, (2) the existence of a diagnosis of hypertension and (3) the administration of treatment for more than one year. An exclusion criterion was the existence of a confirmed mental disorder. The questionnaire was distributed to the participants in paper form in the period April- May 2021. All procedures were performed in accordance with the ethical standards of the 1964 Declaration of Helsinki, as revised in 2000.
Questionnaires
The assessment of the level of compliance with therapeutic treat- ment in elderly hypertensive patients was performed using the Self-Efficacy for Appropriate Medication Use Scale (SEAMS) [17]. The SEAMS scale is a validated self-report scale that mea- sures the patient's confidence in the ability to take appropriate medications. The scale has been shown to exhibit high internal reliability and strong validity [17]. It consists of a total of 16 ques- tions, on a Likert scale (1=Not at all sure, 2=A little sure, 3=Very sure) with a possible range of the total evaluation between 16 and 48. Higher scores indicate better patient self-efficacy in compli- ance with treatment. In addition, apart from these 16 questions, the demographic characteristics of the patients were recorded (gender, age, years since diagnosis, years since treatment, marital status, level of education).
Statistical analysis
Statistical data analysis was performed using statistical analysis software, IBM SPSS version 25. Data analysis was based on de- scriptive statistics indicators, frequencies (ν) or percentage (%) as well as mean (SD) and standard deviation (SD). Inductive statis- tical tests, such as the t-test, for comparison of the mean of two independent samples and the test for comparison of the mean of three or more independent samples one-way ANOVA were used to compare the level of medication compliance with respect to pa- tient demographics. All comparisons were made using a signifi- cance level of α=0.05.
Results
Demographic and occupational data of the sample
The first section of the results chapter presents the findings of the analysis regarding the demographic characteristics of the 73 elder- ly people with hypertension who participated in the research. In total, 51 (69.9%) women and 22 (30.1%) men participated in the present study. The majority of the sample were compulsory edu- cation graduates (n=62, 84.9%) while a smaller percentage of par- ticipation was recorded by patients who were High School gradu- ates (n=11, 15.1%). Finally, 60.3% (n=44) of the participants were widowed and 32.9% (n=24) were married. A smaller percentage of the sample declared themselves single (n=3, 4.1%) and divorced (n=2, 2.7%).
Also, the findings showed that the average age of the sample was 76.7 (SD=9.0) years. In addition, participants had on average been diagnosed with hypertension in the past 16.7 (SD=8.6) years and had been on medication for an average of 16.6 (SD=8.5) years.
In the next section of the results chapter, the findings of the analy- sis are given regarding the level of compliance of the elderly with hypertension with their treatment. The findings are first presented per question of the SEAMS scale and then the overall assessment of the level of compliance of the elderly with hypertension with their treatment is presented. Table 1 presents the findings of the analysis for the individual questions of the SEAMS tool. From the analysis of the 16 questions of the scale, it emerged that 54.8% (n=40) of the elderly stated that they could take their medication correctly even if they took many different medications every day.
In contrast, 31.5% (n=23) of the sample expressed doubts as to whether they would be able to take their medication correctly if they took many different medications every day, while 13.7% (n=10) expressed confidence that they would have a medication compliance problem in this case. The next question aimed to record whether taking medication more than once a day affects medication compliance. From the analysis it emerged that 53.4% (n=39) of the elderly stated that they were sure that they could take their medication correctly even if they took medication more than once a day. On the contrary, a percentage of 31.5% (n=23) of the sample expressed doubts while 15.1% (n=11) declared themselves unable to adhere to the medication in the event that they took med- ication more than once a day. The third question was intended to record whether they could comply with the medication in cases where they are not at home.
The analysis showed that 35.6% (n=26) of the elderly stated that they were sure they could take their medication even if they were away from home, while a percentage of 39.7% (n=29) of the sam- ple stated that there is little certainty as to whether they would be able to adhere to their medication even if they are away from home. Conversely, 24.7% (n=18) stated that they would not be able to comply with medication if they are not at home. The fourth question was intended to capture the extent to which they could comply with medication on a busy day. The analysis showed that 32.9% (n=24) of the elderly stated that they were sure they could take their medication on a busy day, while a percentage of 43.8% (n=32) of the sample stated that they were a little unsure as to whether they would be able to take their medication on a busy day. In contrast, 23.3% (n=17) of participants were certain that a busy day would lead to medication non-compliance.
Table 1: Descriptives of SEAMS questions
|
How confident are you that you can take your medication correctly? |
Not confident at all |
A little confident |
Very confident |
||||
|
ν |
% |
ν |
% |
ν |
% |
||
|
1. |
If you take many different medicines every day |
10 |
13.7% |
23 |
31.5% |
40 |
54.8% |
|
2. |
If you take medicine more than once a day |
11 |
15.1% |
23 |
31.5% |
39 |
53.4% |
|
3. |
If you are not at home |
18 |
24.7% |
29 |
39.7% |
26 |
35.6% |
|
4. |
If you have a busy day |
17 |
23.3% |
32 |
43.8% |
24 |
32.9% |
|
5. |
If the medicines cause any side effects |
22 |
30.1% |
29 |
39.7% |
22 |
30.1% |
|
6. |
If no one reminds you to take your medicine |
17 |
23.3% |
23 |
31.5% |
33 |
45.2% |
|
7. |
If the schedule to take the medicine is not convenient |
17 |
23.3% |
34 |
46.6% |
22 |
30.1% |
|
8. |
If your daily routine breaks down |
17 |
23.3% |
36 |
49.3% |
20 |
27.4% |
|
9. |
If you are not sure how to take the medicine |
16 |
21.9% |
35 |
47.9% |
22 |
30.1% |
|
10. |
If you are not sure what time of day you should take your medicine |
19 |
26.0% |
28 |
38.4% |
26 |
35.6% |
|
11. |
If you feel sick (have a cold or flu) |
13 |
17.8% |
37 |
50.7% |
23 |
31.5% |
|
12. |
If you take your old medicine again and some pills look different than usual |
17 |
23.3% |
31 |
42.5% |
25 |
34.2% |
|
13. |
If the doctor changes your medication |
12 |
16.4% |
29 |
39.7% |
32 |
43.8% |
|
14. |
If you are not sure how the medicine works or what it offers you |
10 |
13.7% |
34 |
46.6% |
29 |
39.7% |
|
15. |
How confident are you that you will be able to pay for your medications? |
16 |
21.9% |
23 |
31.5% |
34 |
46.6% |
|
16. |
How confident are you that you will be able to get to the pharmacy to get your medication? |
24 |
32.9% |
24 |
32.9% |
25 |
34.2% |
The next question was intended to record whether they would be able to comply with the medication if it caused side effects. From the analysis it emerged that 30.1% (n=22) of the elderly stated that they were sure that they could take their medication even if it caused side effects, while a percentage of 39.7% (n=29) of the sample stated that they were not sure if they would be able to stick to the medication if it caused side effects. On the contrary, 30.1% (n=22) of the participants said they were sure that the side effects would lead them to non-compliance with medication.
The sixth question was intended to capture the extent to which they would be able to comply with medication if they did not have someone to remind them. The analysis showed that 45.2% (n=33) of the elderly stated that they were sure they could take their med- ication if they did not have someone to remind them, while a per- centage of 31.5% (n=23) of sample stated that they were not sure if they would be able to adhere to medication if they did not have someone to remind them. On the contrary, 23.3% (n=17) of the participants stated that not being reminded to receive the treatment would definitely lead them to non-compliance.
The next question was intended to capture the extent to which they would be able to comply with the medication if its schedule was inconvenient. From the analysis, it emerged that 30.1% (n=22) of the elderly stated that they were sure that they could take their medication even if the schedule for taking it was not convenient. On the contrary, a percentage of 46.6% (n=34) of the sample stated that an inconvenient schedule would make it difficult for them to comply with a medication, while 23.3% (n=17) of the participants are sure that if the receiving schedule is not convenient will not comply with medication. The eighth question was intended to cap- ture whether older people with hypertension could comply with medication if it disrupted their daily routine. From the analysis, it emerged that 27.4% (n=20) of the elderly stated that they could definitely comply with the medication even if it spoiled their daily routine. On the contrary, a percentage of the order of 49.3% (n=36) of the sample stated that if the medication spoiled their daily rou- tine, it is possible that there would be no compliance with it, while 23.3% (n=17) of the participants stated that it is certain that if the medication disrupted their daily routine they would not comply with the medication.
The next question was intended to capture whether they would be able to comply with the medication if they were not sure how to take the medication. From the analysis it emerged that 30.1% (n=22) of the elderly stated that they were sure that they could take their medication if they were not sure how to take the medication. On the contrary, a percentage of 47.9% (n=35) of the sample stated that if they were not sure how to take the medicine, it is possible that they would not be able to comply with the medication, while 21.9% (n=16) of the participants are sure that if they were not sure how to take the medicine they would not be able to comply with the medication.
The tenth question was intended to capture whether older people with hypertension could comply with medication if they were not sure what time of day they should take their medication. From the analysis it emerged that 35.6% (n=26) of the elderly stated that they could definitely comply with the medication even if they were not sure what time of day they should take the medication. On the contrary, a percentage of 38.4% (n=28) of the sample stated that they would have difficulties in complying with medication if they were not sure what time of day they should take their medication, while 26% (n=19) of of participants stated that they would certain- ly not be able to comply with medication even if they were not sure what time of day they should take the medication. The next ques- tion was intended to capture the extent to which they would be able to comply with medication if they felt ill. The analysis showed that 31.5% (n=23) of the elderly stated that they were sure that they could take their medication even if they felt sick. On the contrary, a percentage of 50.7% (n=37) of the sample stated that they were not sure if they could comply with the medication if they felt sick, while 17.8% (n=13) of the participants said they were sure that they would not be able to comply on medication if they felt ill.
The next question was intended to capture whether the elderly would be able to comply with medication if they were to take their old medication again, and some pills looked different than usu- al. From the analysis it emerged that 23.3% (n=17) of the elderly stated that in this case they would definitely not be able to comply with the medication while 42.5% (n=31) stated that in this case they would not be sure that they can comply with medication. The thirteenth question was intended to capture whether older people with hypertension would be able to comply with medication if the doctor changed their medication. From the analysis it emerged that 43.6% (n=32) of the elderly stated that they could definitely comply with the medication even if the doctor changed their med- ication. On the contrary, a percentage of 39.7% (n=29) of the sam- ple stated that they would have difficulties in complying with the medication if the doctor changed their medications, while 16.4% (n=12) stated that they would definitely not be able to comply on medication even if the doctor changed their medication.
The next question was intended to capture whether the elderly could comply with medication if they were not sure how the med- ication works or did not know what it offers them. The analysis showed that 13.7% (n=10) of the elderly stated that in this case they would definitely not be able to comply with the medication, while 46.6% (n=34) stated that in this case they would not be sure that they can comply with medication. The penultimate question was intended to capture whether the elderly are confident that they can pay for their medications. From the analysis, it emerged that 21.9% (n=16) of the elderly stated that they are not at all sure that they can pay for their medications, while 31.5% (n=23) stated that they have doubts about whether they can pay for their medications. On the contrary, 46.6% (n=34) of the elderly stated that they are sure they can pay for their medicines. The penultimate question was intended to record whether the elderly is confident that they can go to the pharmacy to get their medicines. From the analysis it emerged that 32.9% (n=24) of the elderly stated that they are not at all sure that they can go to the pharmacy to get their medicines while 32.9% (n=24) stated that they have doubts about whether they can to go to the pharmacy to get their medicines. On the con- trary, 34.2% (n=25) of the elderly stated that they are sure that they can go to the pharmacy to get their medicines.
Figure 1 shows the results for the overall assessment of the level of compliance of the elderly with hypertension in their treatment. The findings of the analysis showed that the average value of the elder- ly on the SEAMS scale was found to be equal to 34.6 (TA=8.9). This result shows that elderly people with hypertension have a moderate level of adherence to their medication as the scale can take values between 16 and 48 (interval mean=32).
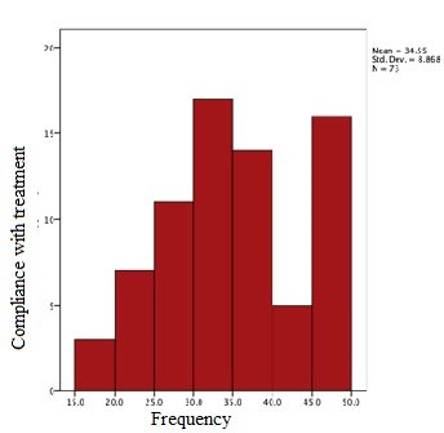
Figure 1: Distribution of overall assessment of treatment compliance
Also, from the analysis it emerged that age (r=-0.322, p=0.005), years since diagnosis (r=-0.289, p=0.015) and years the elderly receive treatment (r=-0.286, p=0.0016) are negatively associated (with a reduced level) of adherence to treatment.
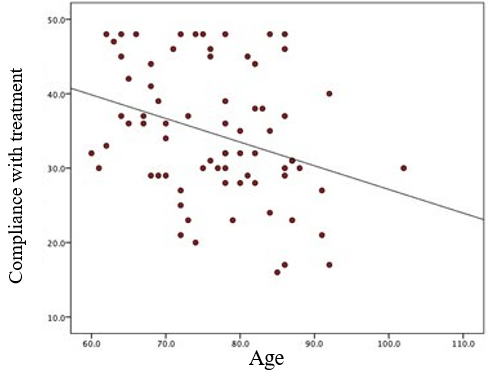
Figure 2: Correlation between age and level of compliance with medication
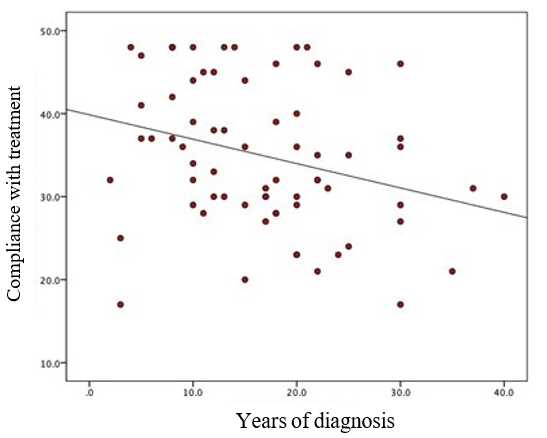
Figure 3: Correlation between years of diagnosis and level of compliance with medication
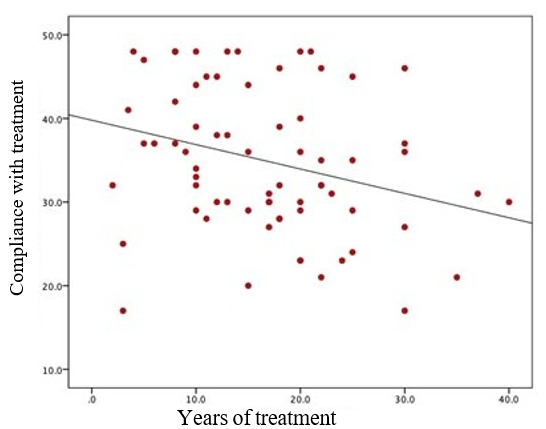
Figure 4: Correlation between years of therapy and level of com- pliance with medication
Discussion
The purpose of the present study was to highlight factors that in- fluence the level of adherence in medication among patients with hypertension. The findings of the analysis showed that age, years since initiation of treatment and years since diagnosis were found to be significant, while gender, education level, and marital status were not confirmed to be associated with the level medication com- pliance. These findings confirm that age and some treatment-relat- ed factors influence the level of medication adherence in elderly patients with hypertension but did not confirm that educational level, gender and marital status influence the level of medication adherence of elderly patients with hypertension [15].
Conclusion
There are several limitations in this study. First, the sample size was not calculated in a rigorous mathematical way given the lack of previous studies in this area. The 73 patients we included in the study, although meeting the condition of n>30 may be underpow- ered to power analyzes to find significant differences and to detect significant associations. Second, the convenience sampling strate- gy may have limited the representativeness of our study sample, as we were only able to reach patients who were easily and im- mediately accessible. The third limitation to the study is potential measurement bias.
Although the adherence scale used in this study has been widely adopted by researchers in other settings, the validity of the mea- sures has never been verified in the context of Greece in a sample of elderly patients. Based on the above limitations, more studies are needed on the level of compliance in the treatment of elderly people with hypertension with a sample selection that will be rep- resentative of the general population. In addition, research is need- ed that will record other possible factors that influence the level of compliance in the treatment of elderly people with hypertension. Such factors may be the level of social support of the elderly from their family/friends, the level of health literacy and the severity/ severity of depressive symptoms. Additionally, an important area of future research is to conduct an experimental study to identify those interventions that can change the behavior of the elderly with hypertension and increase their adherence to treatment.
References
- Uchmanowicz, B., Chudiak, A., Uchmanowicz, I., RosiÅ?czuk, J., & Froelicher, E. S. (2018). Factors influencing adherence to treatment in older adults with hypertension. Clinical inter- ventions in aging, 2425-2441.
- Lim, S. S., Vos, T., Flaxman, A. D., Danaei, G., Shibuya, K., Adair-Rohani, H., Amann, M., Anderson, H. R., Andrews,K. G., Aryee, M., Atkinson, C., Bacchus, L. J., Bahalim, A. N., Balakrishnan, K., Balmes, J., Barker-Collo, S., Baxter, A., Bell, M. L., Blore, J. D., Blyth, F., Memish, Z. A. (2012). A comparative risk assessment of burden of disease and in- jury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet (London, England), 380(9859), 2224–2260.
- Joyce, M., & Hawks, J. H. (2005). Medical-surgical Nursing: Clinical Management for Positive Outcomes. Elsevier Saun- ders.
- Barrera, L. (2018). High Blood Pressure prevention and con- trol: from evidence to action. Colombia Médica, 49(2), 137- 138.
- Kitt, J., Fox, R., Tucker, K. L., & McManus, R. J. (2019). New approaches in hypertension management: a review of current and developing technologies and their potential impact on hy- pertension care. Current hypertension reports, 21(6), 1-8.
- He, W., Bonner, A., & Anderson, D. (2016). Patient report- ed adherence to hypertension treatment: a revalidation study. European Journal of Cardiovascular Nursing, 15(2), 150-156.
- Kleinsinger, F. (2018). The unmet challenge of medication nonadherence. The Permanente Journal, 22.
- Mancia, G., Fagard, R., Narkiewicz, K., Redón, J., Zanchetti, A., Böhm, M., Christiaens, T., Cifkova, R., De Backer, G., Dominiczak, A., Galderisi, M., Grobbee, D. E., Jaarsma, T., Kirchhof, P., Kjeldsen, S. E., Laurent, S., Manolis, A. J., Nils- son, P. M., Ruilope, L. M., Schmieder, R. E., … Task Force Members (2013). 2013 ESH/ESC Guidelines for the manage- ment of arterial hypertension: the Task Force for the manage- ment of arterial hypertension of the European Society of Hy- pertension (ESH) and of the European Society of Cardiology (ESC). Journal of hypertension, 31(7), 1281–1357.
- Vrijens, B., Antoniou, S., Burnier, M., De la Sierra, A., & Volpe, M. (2017). Current situation of medication adherence in hypertension. Frontiers in pharmacology, 8, 100.
- Uchmanowicz, B., Jankowska, E. A., Uchmanowicz, I., & Morisky, D. E. (2019). Self-reported medication adherence measured with morisky medication adherence scales and its determinants in hypertensive patients aged≥ 60 years: a sys- tematic review and meta-analysis. Frontiers in Pharmacology, 10, 168.
- Alhaddad, I. A., Hamoui, O., Hammoudeh, A., & Mallat, S. (2016). Treatment adherence and quality of life in patients on antihypertensive medications in a Middle Eastern population: adherence. Vascular health and risk management, 12, 407.
- Cummings, D. M., Wu, J. R., Cene, C., Halladay, J., Dona- hue, K. E., Hinderliter, A., ... & DeWalt, D. (2016). Perceived social standing, medication nonadherence, and systolic blood pressure in the rural south. The Journal of Rural Health, 32(2), 156-163.
- Li, Y. T., Wang, H. H., Liu, K. Q., Lee, G. K., Chan, W. M.,Griffiths, S. M., & Chen, R. L. (2016). Medication adherence and blood pressure control among hypertensive patients with coexisting long-term conditions in primary care settings: a cross-sectional analysis. Medicine, 95(20).
- Jankowska-PolaÅ?ska, B., Dudek, K., Szymanska-Chabowska, A., & Uchmanowicz, I. (2016). The influence of frailty syn- drome on medication adherence among elderly patients with hypertension. Clinical Interventions in Aging, 11, 1781.
- Jackevicius, C. A., Mamdani, M., & Tu, J. V. (2002). Adher- ence with statin therapy in elderly patients with and without acute coronary syndromes. Jama, 288(4), 462-467.
- Lam, P. W., Lum, C. M., & Leung, M. F. (2007). Drug non-ad- herence and associated risk factors among Chinese geriatric patients in Hong Kong. Hong Kong Medical Journal, 13(4), 284.
- Risser, J., Jacobson, T. A., & Kripalani, S. (2007). Develop- ment and psychometric evaluation of the Self-efficacy for Ap- propriate Medication Use Scale (SEAMS) in low-literacy pa- tients with chronic disease. Journal of nursing measurement, 15(3), 203-219.