


Research Article - (2025) Volume 10, Issue 1
A Comparative Study of Ultrasound-Guided Infraclavicular Block with Bupivacaine Alone or Bupivacaine Combined with Dexmedetomidine for Postoperative Analgesia in Upper Limb Surgeries
2Department of Anaesthesia, Shardaben General Hospital, NHLMMC, Ahmedabad, Gujarat, India
Received Date: Jan 24, 2025 / Accepted Date: Feb 27, 2025 / Published Date: Mar 17, 2025
Copyright: ©Â©2025 Dr. Vismit Gami, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Vasava, V. G., Shah, S., Satasia, J. R., Gami, V. (2025). A Comparative Study of Ultrasound-Guided Infraclavicular Block with Bupivacaine Alone or Bupivacaine Combined with Dexmedetomidine for Postoperative Analgesia in Upper Limb Surgeries. J Anesth Pain Med, 10(1), 01-06.
Abstract
This study aimed to compare the efficacy of ultrasound-guided infraclavicular block using Bupivacaine alone versus Bupivacaine combined with Dexmedetomidine for postoperative analgesia in upper limb surgeries. A total of 60 patients were randomly divided into two groups: Group A received 0.5% Bupivacaine, and Group B received 0.5% Bupivacaine with 0.75 μg/kg Dexmedetomidine. The primary outcomes measured were the onset and duration of sensory and motor block, as well as the duration of analgesia. Results showed that Group B had a significantly faster onset and longer duration of sensory and motor block, as well as prolonged analgesia compared to Group A. No complications were observed in either group. These findings suggest that the addition of Dexmedetomidine improves the effectiveness of infraclavicular blocks for postoperative analgesia.
Keywords
Infraclavicular Block, Dexmedetomidine, Bupivacaine, Ultrasound-Guided Anesthesia, Postoperative Analgesia.Introduction
Peripheral nerve block not only provide excellent intraoperative analgesia but also provide good postoperative analgesia, reduction in stress response and systemic analgesic requirements.
Upper limb surgery is mostly performed under brachial plexus block which are given by various approaches, one of which is infraclavicular block for anaesthesia and analgesia for upper limb surgeries.
Various adjuvant like Dexamethasone, Dexmedetomidine, clonidine is used to prolong duration of analgesia of nerve block.
Aims and Objectives
This study was conducted to compare and evaluate effect of Dexmedetomidine as an adjuvant to Bupivacaine alone in infraclavicular brachial plexus block for upper limb surgery. Patients were observed for following parameters
Primary Objective
• Total duration of analgesia in both groups
Secondary Objective
• Onset and duration of sensory block
• Onset and duration of motor block
• Complications
Methodology
A prospective observational study was conducted at Smt. Shardaben General Hospital, Ahmedabad, after obtaining approval from the hospital's Institutional Review Board (IRB). The study enrolled 60 patients, aged 18 to 60 years, with an American Society of Anesthesiologists (ASA) physical status classification of grade I or II, who were scheduled to undergo upper limb surgeries.
Exclusion Criteria
Patients with ASA grade III or higher, pregnant females, individuals with bleeding disorders, those with known hypersensitivity to local anesthetics or adjuvants, patients with preexisting neuropathy, and those with a local infection at the proposed injection site were excluded from the study.
Preoperative Protocol
All participants underwent a pre anesthetic evaluation, and the procedure was thoroughly explained to them one day prior to surgery. Patients were instructed to remain nil by mouth overnight prior to the procedure. In the operating theatre, a 20G intravenous cannula was inserted, and baseline measurements of pulse, blood pressure, oxygen saturation, and respiratory rate were recorded.
Study Groups
Patients were randomly assigned into two groups, with 30 patients in each group.
• Group A: 25 ml of 0.5% Bupivacaine (dose not exceeding the toxic limit of 3 mg/kg of the drug).
• Group B: 25 ml of 0.5% Bupivacaine with 0.75 µg/kg of Dexmedetomidine.
The randomized allocation ensured the study's impartiality and aimed to assess the comparative effectiveness of the two anesthetic regimens.
Technique
Under all aseptic precautions and patients in supine position, their head turned away from the side to be blocked and arm abducted at 90°. The high frequency probe of ultrasound machine (8-12 MHz) was positioned in parasagital plane just medial to coracoid process and inferior to clavicle.
After locating Axillary artery and vein just beneath sheath of pectoralis minor muscle and medial ,lateral and posterior cords appearing caudal , cephalic and posterior to the artery , respectively are located.
After aspiration to avoid unintentional intra vascular injection, test dose of 1-2 ml of 1% lidocaine and epinephrine, followed by loading dose of local anaesthetic administered


Ultrasound Image of Infraclavicular Brachial Plexus AA-Axillary Artery, AV-Axillary Vein, LC-Lateral Cord, PC-Posterior Cord, MC- Medial Cord

Modified Bromage Scale
Duration of Analgesia
The duration of analgesia was defined as the time from the onset of Grade 1 sensory block to the requirement for the first dose of rescue analgesia.
Postoperative Monitoring
Postoperative monitoring was conducted at the following intervals:
• Every 30 minutes for the first 6 hours.
• Every hour from 6 to 10 hours.
• Every 2 hours until 24 hours post-surgery.
The postoperative duration of sensory block, motor block, and analgesia was assessed. Patients were also evaluated using the Visual Analogue Scale (VAS) for pain assessment.
VAS Score
Postoperative pain intensity was assessed using the Visual Analogue Scale (VAS), which is a commonly used method for quantifying pain levels in patients.

VAS Score Chart
Statistical Analysis
Descriptive data of both the groups were compared using unpaired t’ tests. ‘P’ value <0.05 was considered statistically significant and <0.001 was considered highly significant.

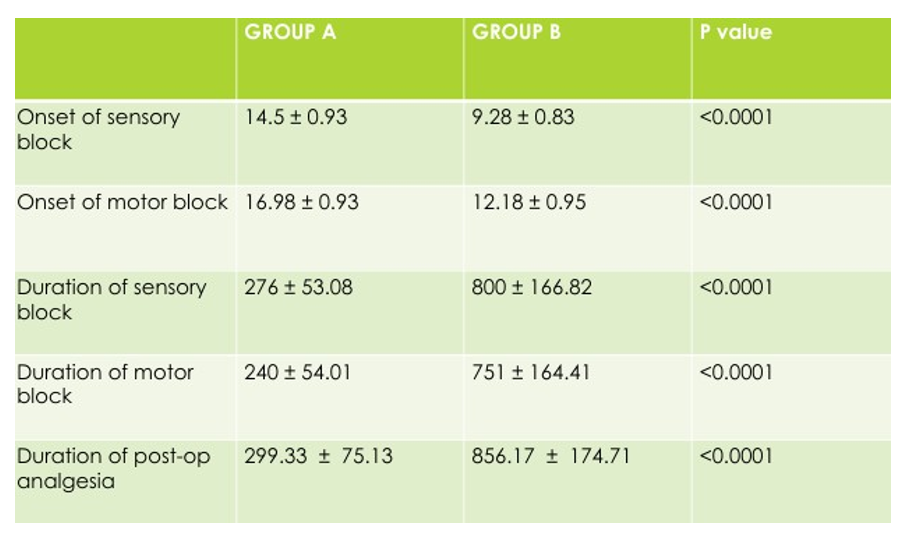
Comparison of Mean Sensory and Motor Onset
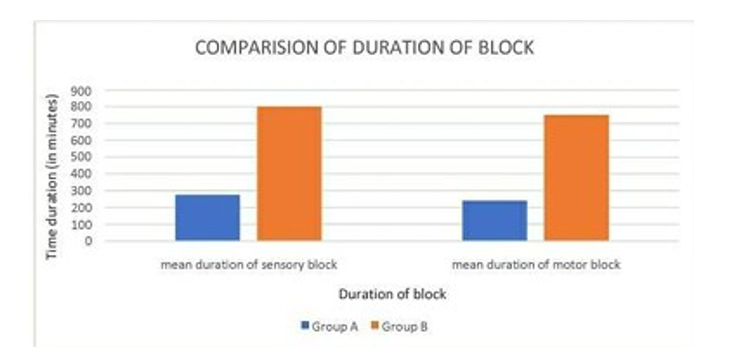
Comparision of Duration of Sensosry and Motor Blockade
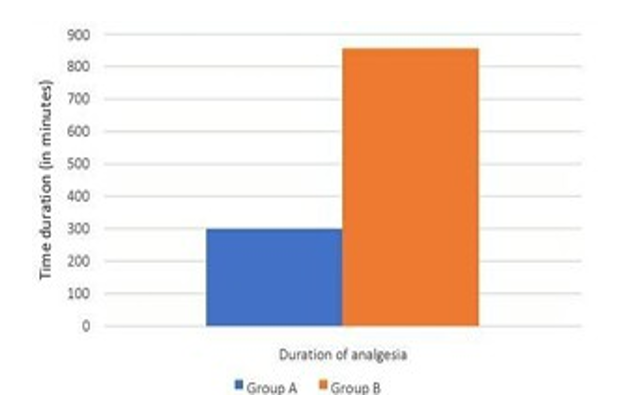
Comparison of Duration of Post-Op Analgesia
Results
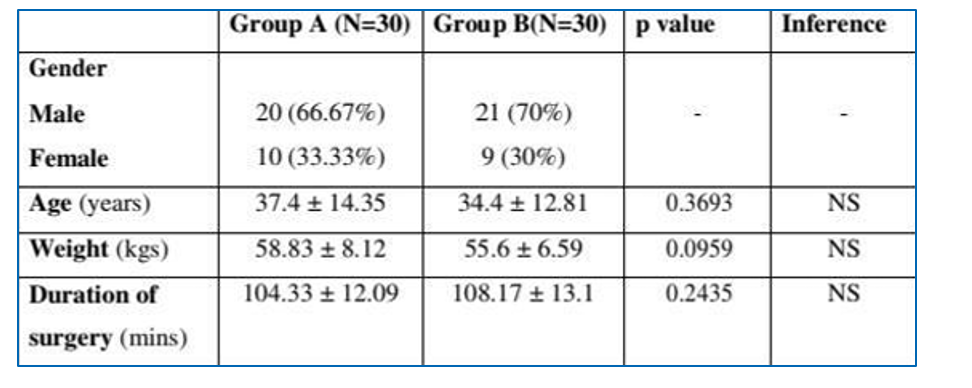
Demographic data
Discussion
In our study, the total duration of analgesia in Group A was 299.33 ± 75.13 minutes, while in Group B it was 856.17 ± 174.71 minutes.
Ahmed A. Metwally et al. (14), in their study on infraclavicular block, used a control group with 0.5% Bupivacaine and another group with 100 µg of Dexmedetomidine combined with Bupivacaine. They observed that the total duration of analgesia in the control group was 246.3 ± 35.5 minutes, while in the group with Dexmedetomidine as an adjuvant, it was 809.2 ± 95.8 minutes. These findings are similar to our study.
Khaled M. Mahmoud (10) observed that the duration of analgesia in the group using plain Bupivacaine for an infraclavicular block was 255 ± 126 minutes. However, they used 0.325% Bupivacaine (30 ml) in their study.
It is evident that Group B, receiving the adjuvant Dexmedetomidine, demonstrated a faster onset of sensory and motor block, longer duration of both sensory and motor block, and a prolonged duration of analgesia compared to Group A, which received only plain Bupivacaine without any adjuvant.
Conclusion
This study concludes that the onset of sensory and motor block is significantly faster in the Dexmedetomidine group compared to the plain Bupivacaine group. The duration of both sensory and motor block is significantly longer with the addition of Dexmedetomidine as an adjuvant. Additionally, the duration of analgesia is significantly extended in the Dexmedetomidine group compared to Bupivacaine alone.
The use of ultrasound guidance, in addition to improving the success rate, also reduces complications such as accidental arterial puncture, Horner’s syndrome, and pneumothorax. No complications were observed in this study.
References
- Mahmoud, K. M., & Ammar, A. S. (2011). Ultrasound- guided continuous infraclavicular brachial plexus block using bupivacaine alone or combined with adenosine for pain control in upper limb surgery. Saudi Journal of Anaesthesia, 5(2), 132-137.
- RcajoPmPb. iHniestdoricwaitlhaspect of regional anaesthesia. 1st ed. Chapter 1. In: Text bookof Regional Anaesthesia; 2002 May.p.3.
- Ammar, A. S., & Mahmoud, K. M. (2012). Ultrasound-guided single injection infraclavicular brachial plexus block using bupivacaine alone or combined with dexmedetomidine for pain control in upper limb surgery: A prospective randomized controlled trial. Saudi journal of anaesthesia, 6(2), 109-114.
- KAhparlidl-juMne. M20o1h2m: o1u09d-,11A4m. ay S. Ammar. Ultrasound guided continous
- infraclavicular brachial plexus block using bupivacainealone or combined with adenosine for pain control in upper limb surgery ,Saudi journal of anaesthesia. Vol 5. April-june 2011,5,132-137.
- Sandhu, N. S., & Capan, L. M. (2002). Ultrasound-guided infraclavicular brachial plexus block. British journal of anaesthesia, 89(2), 254-259.
- El-Hennawy, A. M., Abd-Elwahab, A. M., El-Ozairy, H. S. et al. (2017). Dexmedetomidine as an Adjuvant to Bupivacaine in Infraclavicular Brachial Plexus Block: A Prospective Randomized Controlled Trial. Saudi Journal of Anesthesia, 11(3), 257-263.
- Esmaoglu, A., Yegenoglu, F., Akin, A., & Turk, C. Y. (2010). Dexmedetomidine added to levobupivacaine prolongs axillary brachial plexus block. Anesthesia & Analgesia, 111(6), 1548- 1551.
- Kaabachi, O., Ben, G. M., Ghachem. R. et al. (2015). Dexmedetomidine as an Adjuvant to Bupivacaine in Infraclavicular Brachial Plexus Block: A Randomized Controlled Trial. Journal of Anesthesia, 29(5), 645-651.