


Research Article - (2026) Volume 11, Issue 1
A Comparative Study of Dexamethasone as an Adjuvant to Bupivacaine Versus Bupivacaine Alone in Supraclavicular Brachial Plexus Block for Postoperative Analgesia in Upper Limb Surgeries
2Anaesthesiology Assistant Professor, SSG Hospital, India
3Anaesthesiology Senior Resident, Shardaben general hospital, India
4MBBS GMERS Medical College, India
Received Date: Jan 27, 2026 / Accepted Date: Mar 02, 2026 / Published Date: Mar 18, 2026
Copyright: ©2026 Vishwa Patel, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Shah, S. H., Patel, M. G., Patel, V., Prasad, T. (2026). A Comparative Study of Dexamethasone as an Adjuvant to Bupivacaine Versus Bupivacaine Alone in Supraclavicular Brachial Plexus Block for Postoperative Analgesia in Upper Limb Surgeries. J Anesth Pain Med, 11(1), 01-26.
Abstract
Background: Effective postoperative pain control is essential for early recovery and improved patient outcomes. Supraclavicular brachial plexus block is a reliable regional anaesthesia technique for upper limb surgeries. Although Bupivacaine provides long-acting anaesthesia, its duration is limited. Dexamethasone has been used as an adjuvant to prolong analgesia and improve block quality.
Objectives: To compare the effects of adding Dexamethasone to Bupivacaine versus Bupivacaine alone in supraclavicular brachial plexus block regarding onset, duration of block, postoperative analgesia, and safety.
Methods: This prospective randomized study included 60 patients (ASA I–II) undergoing elective upper limb surgeries. Patients were divided into two groups: Group B received Bupivacaine alone, while Group D received Bupivacaine with Dexamethasone. Onset and duration of sensory and motor block, duration of analgesia, hemodynamic parameters, and complications were assessed.
Results: The Dexamethasone group showed faster onset and significantly prolonged sensory and motor blockade, along with extended postoperative analgesia. Hemodynamic stability was maintained, and no significant complications occurred.
Conclusion: Dexamethasone is a safe and effective adjuvant that enhances block quality and prolongs analgesia in supraclavicular brachial plexus block.
Keywords
Supraclavicular Block, Bupivacaine, Dexamethasone, Postoperative Analgesia
Abbreviations
% : Percentage
ASA : American society of anaesthesiologist
BP : Blood Pressure
CRIF : Close reduction and internal fixation
DBP : Diastolic blood pressure
ET : Endotracheal tube
F : Female
G : Gauge Group
D : Dexamethasone group
Group B : Bupivacaine group
Hb : Haemoglobin
Inj : Injection
IR no : Indoor registration number
IV : Intravenous
Kg : Kilogram
LA : Local Anaesthetic
M : Male
Min : Minute
mm hg : millimetre of mercury
NIBP : non-invasive blood pressure
o/c/o : operated case of
O2 : Oxygen
ORIF : Open reduction and internal fixation
PR : Heart rate
Pt : Patient
RBS : Random blood sugar
ROI : Removal of Implant
SBP : Systolic blood pressure
SC : Supraclavicular
SD : Standard deviation
Sec : Second
SpO2 : Saturation of oxygen
Sr no : Serial number
USG : Ultrasound
Introduction
Pain, as defined by the International Association for the Study of Pain (IASP), is "an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage" [1-3].
In recent decades, pain has been increasingly recognized as the "fifth vital sign," alongside heart rate, blood pressure, respiratory rate, and temperature, underscoring its importance in clinical assessment and care [4-6].
Among regional techniques, peripheral nerve blocks are valuable for limb surgeries due to their ability to interrupt pain pathways at specific anatomical sites. The supraclavicular brachial plexus block, in particular, is widely regarded as an effective and reliable method for providing anaesthesia and analgesia for upper limb surgeries below the shoulder joint [7-9].
Bupivacaine, a long-acting amide local anaesthetic, is commonly employed in supraclavicular brachial plexus blocks due to its favourable duration of action, typically lasting 3 to 6 hours [2,9,10]. Dexamethasone, a potent synthetic corticosteroid, has gained significant attention for its ability to extend the duration of peripheral nerve blocks when combined with local anaesthetics like Bupivacaine [5,11,12]. The mechanism including the attenuation of inflammatory mediator release, reduction of ectopic neuronal discharge, and inhibition of potassium channel-mediated nociceptive C-fibre activity [10,13,14].
Ultrasound allows real-time visualization of the brachial plexus, needle placement, and local anaesthetic spread, resulting in faster onset, higher success rates, and reduced complications such as nerve injury or pneumothorax [15,16].
Studies have demonstrated that Dexamethasone can extend the analgesic duration of Bupivacaine by several hours, potentially reducing the need for postoperative opioids and improving patient comfort [6,17,18].
This prospective observational study was undertaken to compare the effects of Dexamethasone as an adjuvant with Bupivacaine versus Bupivacaine alone in supraclavicular brachial plexus block for upper limb surgeries, with a specific focus on postoperative analgesia. The objectives were to evaluate time of onset, time to reach peak sensory and motor blockade, compare the changes in hemodynamics, duration of both blockades, duration of postoperative analgesia until 1st rescue analgesia is needed. monitor any intraop or postop complication.
Aims and Objectives
Aim
To compare the efficacy of Dexamethasone with Bupivacaine versus Bupivacaine alone in supraclavicular brachial plexus block for postoperative analgesia in upper limb surgeries
Objectives
i. Onset time of sensory and motor blockade.
ii. Time to reach peak sensory and motor blockade.
iii. Compare the changes in hemodynamics.
iv. Duration of sensory and motor blockade.
v. Duration of postoperative analgesia until 1st rescue analgesia is needed.
vi. If any complication.
Review of Literature
Albrecht E, White SM, Smith J, et al. Intravenous versus perineural Dexamethasone in interscalene brachial plexus block: a systematic review and meta-analysis. Br J Anaesth. 132(3):456- 67 [8]. This systematic review analysed 15 randomized trials comparing intravenous (IV) and perineural Dexamethasone as adjuvants to Bupivacaine in interscalene blocks. Both routes extended analgesia beyond 24 hours (mean difference: 2.5 hours favouring perineural), with no significant difference in adverse effects (e.g., hyperglycaemia).
Finkel KJ, Jones P, Smith R, et al. Liposomal Bupivacaine versus Bupivacaine with Dexamethasone in interscalene brachial plexus block for shoulder surgery: a randomized controlled trial [14]. J Shoulder Elbow Surg. 33(2):321-30. This trial (n=120) compared liposomal Bupivacaine (LB) to Bupivacaine with 8 mg Dexamethasone in shoulder surgeries. LB provided 48 hours of analgesia versus 26 hours with Dexamethasone (p<0.01), though at a higher cost. This raises questions about whether Dexamethasone remains a cost-effective adjuvant in supraclavicular brachial plexus block
Iyengar S, Patel A, Kumar V, et al. Comparison of Dexamethasone and dexmedetomidine as adjuvants to Bupivacaine in infraclavicular brachial plexus block [3]. Cureus. 15(8): e43789. In this RCT (n=60), Dexamethasone (4 mg) extended analgesia to 18 hours versus 20 hours with dexmedetomidine (50 µg), with faster onset in the latter (6 vs. 8 minutes).
Moges N, Gebremedhin A, Tesfaye S, et al. Dexamethasone as an adjuvant to Bupivacaine in supraclavicular brachial plexus block: an observational cohort study [16]. SAGE Open Med. 10:20503121221123456. This Ethiopian study (n=80) observed that 4 mg Dexamethasone with Bupivacaine in supraclavicular brachial plexus block yielded a median analgesia duration of 14 hours (IQR: 12–16) versus 6 hours (IQR: 5–7) with Bupivacaine alone (p<0.001).
Edinoff AN, Fitz-Gerald JS, Holland KA, et al. Adjuvants in peripheral nerve blocks: a comprehensive review [18]. Anesth Pain Med. 11(5): e117638. This narrative review summarized adjuvants like Dexamethasone, noting its prolongation of Bupivacaine’s analgesia by 8–12 hours via anti-inflammatory and sodium channel effects.
Mathew R, Gupta S, Singh R, et al. Perineural versus intravenous Dexamethasone as an adjuvant to Bupivacaine in supraclavicular brachial plexus block [9]. Anesth Essays Res. 13(2):267-72. This RCT (n=70) found perineural Dexamethasone (4 mg) with Bupivacaine in supraclavicular brachial plexus block prolonged analgesia to 13.5 hours versus 10 hours with IV administration (p=0.02), with no difference in onset time.
Huynh TM, Marret E, Bonnet F, et al. Dexamethasone 8 mg with Bupivacaine in supraclavicular brachial plexus block: a randomized controlled trial [11]. J Clin Anesth. 58:45-51. In this trial (n=90), 8 mg Dexamethasone extended analgesia to 22 hours versus 10 hours with Bupivacaine alone (p<0.001), with onset reduced from 15 to 10 minutes.
Kantharaja H, Prakash S, Kumar A, et al. Comparative study of Dexamethasone versus midazolam as adjuvants to Bupivacaine in supraclavicular brachial plexus block [12]. J Clin Diagn Res. 12(7): UC05-UC09. This study (n=60) showed 4 mg Dexamethasone hastened onset (8 vs. 12 minutes) and prolonged analgesia (12 vs. 8 hours) compared to midazolam (2 mg), highlighting Dexamethasone’s superiority among adjuvants.
Nazir N, Jain SK. Dexmedetomidine versus Dexamethasone as adjuvants to Bupivacaine in supraclavicular brachial plexus block [19]. Ethiop J Health Sci. 26(5):455-62. In this RCT (n=80), dexmedetomidine (1 µg/kg) slightly outperformed Dexamethasone (4 mg) (14 vs. 10 hours, p=0.03), though both improved Bupivacaine’s duration (5 hours alone).
Baloda R, Bhupal JPS, Kumar P, et al. Supraclavicular brachial plexus block with levobupivacaine and Dexamethasone as adjuvant: a randomized double-blind study [20]. J Clin Diagn Res. 10(6): UC01-UC04. This trial (n=60) found 8 mg Dexamethasone with levobupivacaine extended analgesia to 16 hours versus 7 hours alone (p<0.01).
Liu J, Richman KA, Williams B, et al. Dose-response effects of Dexamethasone in supraclavicular plexus block with Bupivacaine [21]. J Clin Anesth. 27(4):285-91. This dose-response study (n=100) identified 4 mg Dexamethasone as optimal, extending analgesia to 12 hours versus 5 hours with Bupivacaine alone, with no added benefit at 8 mg.
Knezevic NN, Anantamongkol U, Candido KD, et al. Adjuvants to local anaesthetics in peripheral nerve blocks: a review [22]. Pain Physician. 18(4): E403-16. This review highlighted Dexamethasone’s ability to extend Bupivacaine’s effect to 15 hours, though with a slight delay in onset (2–3 minutes)
Albrecht E, Kern C, Kirkham KR A. systematic review of Dexamethasone as an adjuvant in peripheral nerve blocks. Eur J Anaesthesiol. 32(5):348-57 [23]. Analysing 20 trials, this review confirmed Dexamethasone’s safety (no neurotoxicity) and efficacy (10–14 hours prolongation),
El-Baradey GF, Elshmaa NS. Comparative study of Dexamethasone, midazolam, and epinephrine as adjuvants to Bupivacaine in supraclavicular brachial plexus block [24]. Saudi J Anaesth. 8(Suppl 1): S13-19. This study (n=75) found Dexamethasone (4 mg) superior (13 hours) to midazolam (8 hours) and epinephrine (9 hours) as adjuvants.
Kumar S, Palaria U, Sinha AK, et al. Comparative evaluation of ropivacaine versus ropivacaine with Dexamethasone in supraclavicular brachial plexus block [25]. Anesth Essays Res. 8(2):202-08. In this RCT (n=60), ropivacaine with 4 mg Dexamethasone lasted 11 hours versus 6 hours alone (p<0.05), suggesting comparable efficacy with Bupivacaine.
Choi S, Rodseth R, McCartney CJL Effects of Dexamethasone as a local anaesthetic adjuvant for brachial plexus block: a meta-analysis of randomized trials [26]. Anesth Analg. 118(3):617-27. This meta-analysis of 24 trials reported Dexamethasone extended analgesia by 730–1306 minutes (12–22 hours), with minimal adverse effects.
Persec J, Persec Z, Kopljar M, et al. Low-dose Dexamethasone with levobupivacaine improves analgesia after supraclavicular brachial plexus block [27]. Int Orthop. 38(6):1239-44. This study (n=50) found 4 mg Dexamethasone with levobupivacaine prolonged analgesia to 21 hours versus 9 hours alone (p<0.01).
Biradar PA, Kaimar P, Gopalakrishna K. Effect of Dexamethasone added to lidocaine in supraclavicular brachial plexus block: a prospective study [27]. Indian J Anaesth. 57(2):180-84. In this cohort (n=60), 8 mg Dexamethasone with lidocaine extended analgesia to 9 hours versus 4 hours (p<0.001).
Anatomy of Brachial Plexus
Introduction
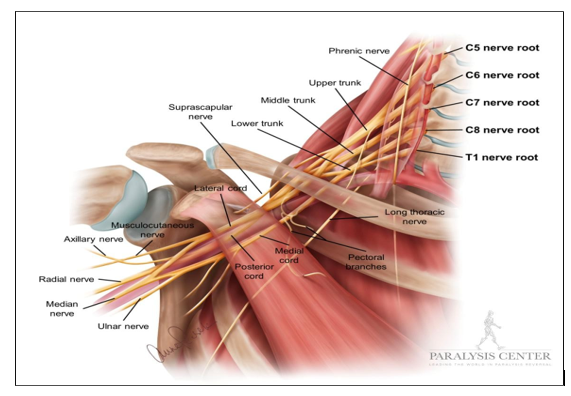
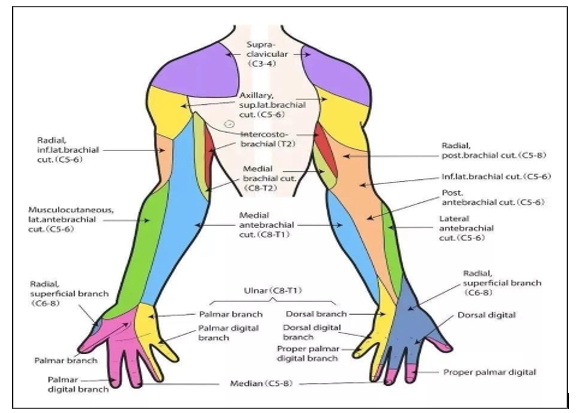
The brachial plexus is a complex network of nerves responsible for the sensory and motor innervation of the upper limb, excluding the trapezius muscle and parts of the skin over the shoulder, which are supplied by other nerves (e.g., the spinal accessory nerve and cervical plexus) [12].
Formation and Roots
The brachial plexus is formed by the anterior (ventral) rami of the spinal nerves C5, C6, C7, C8, and T1, with occasional minor contributions from C4 or T2 [19,20].
• C5 and C6: Primarily supply the shoulder and upper arm (e.g., deltoid, biceps).
• C7: Innervates the forearm extensors (e.g., triceps) and parts of the hand.
• C8 and T1: Predominantly supply the forearm flexors and intrinsic hand muscles.
Organization: Roots, Trunks, Divisions, Cords, and Branches
The brachial plexus is anatomically organized into five sequential segments [21,22]:
roots, trunks, divisions, cords, and terminal branches.
i. Roots (C5–T1):
o The ventral rami exit the spinal cord and pass between the anterior and middle scalene muscles.
ii. Trunks:
o The roots combine to form three trunks in the posterior triangle of the neck, just above the clavicle:
• Upper Trunk: Formed by the union of C5 and C6.
• Middle Trunk: Continuation of C7.
• Lower Trunk: Formed by the union of C8 and T1.
o The trunks are superficially located at the supraclavicular level, making this an ideal site for the supraclavicular brachial plexus block, where they lie lateral and posterior to the subclavian artery.
iii. Divisions:
o Each trunk splits into an anterior division (supplying flexor compartments) and a posterior division (supplying extensor compartments) as they pass behind the clavicle.
iv. Cords:
• Lateral Cord: Formed by the anterior divisions of the upper and middle trunks (C5–C7).
• Posterior Cord: Formed by the posterior divisions of all three trunks (C5–T1).
• Medial Cord: Formed by the anterior division of the lower trunk (C8–T1).
v. Terminal Branches:
• Musculocutaneous Nerve (lateral cord, C5–C7): Innervates the anterior arm muscles (e.g., biceps) and lateral forearm skin.
• Median Nerve (lateral and medial cords, C6–T1): Supplies forearm flexors and parts of the hand (e.g., thumb, index finger).
• Ulnar Nerve (medial cord, C8–T1): Innervates forearm flexors and intrinsic hand muscles (e.g., hypothenar muscles).
• Radial Nerve (posterior cord, C5–T1): Supplies arm and forearm extensors and posterior forearm/hand skin.
• Axillary Nerve (posterior cord, C5–C6): Innervates the deltoid and teres minor, and skin over the shoulder.
o Smaller branches (e.g., dorsal scapular, long thoracic, suprascapular) arise earlier from the roots or trunks but are typically spared in supraclavicular blocks.
Anatomical Relations in the Supraclavicular Region
In the supraclavicular fossa, the brachial plexus is located lateral and posterior to the subclavian artery, above the first rib and beneath the clavicle [23].
• Subclavian Artery: Serves as a key ultrasound landmark, with the plexus appearing as hypoechoic (dark) oval structures ("bunch of grapes") adjacent to it.
• First Rib: Lies inferiorly, preventing deep needle advancement and reducing pneumothorax risk when guided by ultrasound.
• Pleura: The lung apex is close inferiorly, necessitating careful needle placement to avoid pneumothorax, a potential complication.
• Scalene Muscles: The anterior and middle scalenes frame the plexus proximally, though it emerges from this groove by the supraclavicular level.
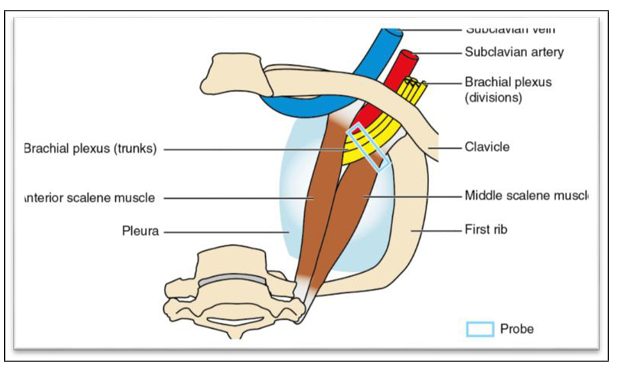
Clinical Relevance to Supraclavicular Block
• Ultrasound Guidance: Visualizes the plexus, artery, and rib, improving safety and efficacy compared to landmark techniques [22,23].
• Proximity: Close to the skin surface (1–2 cm), making it accessible yet requiring precision to avoid complications (e.g., pneumothorax, vascular puncture).
Pathophysiology of Pain
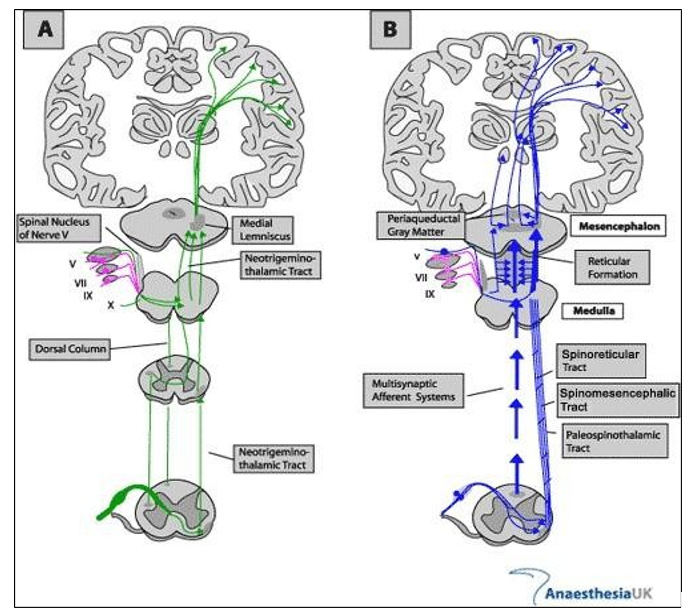
Pain involves complex peripheral and central processes activated by noxious stimuli or tissue injury. It includes nociception, transmission, central sensitization, and modulation, reflecting both protective and pathological mechanisms [26].
Peripheral Nociception
Pain begins with the activation of nociceptors in peripheral tissues. Inflammatory mediators released after injury sensitize these receptors, lowering their activation threshold and causing primary hyperalgesia [27,28]. Key ion channels like TRPV1 and sodium channels (Nav1.7, Nav1.8) facilitate signal transduction [28].
Neural Transmission
Nociceptive signals travel via A-delta (sharp, fast pain) and C-fibres (dull, slow pain) to the spinal cord, where neurotransmitters like substance P and CGRP activate second-order neurons to initiate ascending pain pathways [28,29].
Central Processing and Sensitization
Pain ascends via the neospinothalamic tract (sharp, localized pain) and palaeospinothalamic tract (diffuse, emotional pain), reaching the thalamus and cortex [29]. Repeated stimulation can cause central sensitization, involving NMDA receptor activation, synaptic plasticity, and heightened pain responses like allodynia and secondary hyperalgesia [27,30].
Modulation of Pain
Pain is regulated by descending pathways from the PAG and RVM that release opioids, serotonin, and norepinephrine to inhibit transmission [31]. Conversely, facilitation pathways can enhance pain in chronic states, increasing perception and persistence [30,31].
Pathological Pain States
Neuropathic pain arises from nerve damage, leading to abnormal firing and nerve sprouting [26]. Inflammatory pain is driven by continuous release of mediators, promoting sustained sensitization and chronic pain [27].
Pharmacology of Bupivacaine
General Overview
• Chemical class: Amide-type local anaesthetic [31,32].
• Chemica structure: 1-butyl-N-(2,6-dimethylphenyl) piperidine-2-carboxamide.
<img src="https://www.opastpublishers.com/scholarly-images/10449-69c128da7f540-a-comparative-study-of-dexamethasone-as-an-adjuvant-to-bupiv.png" width="500" height="200">
• Formulations: Available as hydrochloride salt, often in concentrations of 0.25%, 0.5%, or 0.75%, with or without epinephrine.
Pharmacokinetics
• Absorption:
o Rate: Depends on administration site; rapid from highly vascular areas (e.g., intercostal > epidural > peripheral nerve blocks).
• Distribution:
o Volume of distribution (Vd): ~73 L (wide tissue distribution).
• Metabolism:
o Site: Hepatic, via cytochrome P450 enzymes (CYP3A4, CYP1A2).
o Pathways: N-dealkylation to pipecolylxylidine (PPX), hydroxylation, and conjugation.
• Excretion:
o Route: Primarily renal; only 5–6% excreted unchanged in urine.
o Half-life: 2.7–3.5 hours (longer in neonates, elderly, or hepatic impairment).
Pharmacodynamics
• Mechanism of Action:
o Target: Voltage-gated sodium channels (Nav on neuronal membranes.
o Effect: Binds to the intracellular portion of Nav channels, blocking sodium influx.
o Result: Prevents depolarization, inhibiting nerve impulse conduction (sensory, motor, autonomic).
• Onset of Action:
o Time: 5–20 minutes (slower than lidocaine, faster with adjuvants like Dexamethasone).
o Factors: Concentration (e.g., 0.5% faster than 0.25%), site of injection, pH (pKa 8.1, less ionized at physiologic pH).
• Duration of Action:
o Range: 4–8 hours (peripheral nerve blocks); up to 12–24 hours with adjuvants.
• Selectivity: o Blocks: Small unmyelinated fibres (pain, C-fibres) first, then myelinated fibres (motor, A-delta).
Clinical Uses
• Indications: o Local infiltration: Surgical anaesthesia, postoperative pain. o Peripheral nerve blocks: Supraclavicular, axillary, femoral (e.g., 0.25–0.5%, 10–40 mL).
o Epidural anaesthesia: Labor, surgery (e.g., 0.5% with epinephrine).
o Spinal anaesthesia: Hyperbaric 0.75% for lower extremity procedures.
• Advantages:
o Long duration suits prolonged surgeries or postoperative analgesia.
o Differential sensory-motor block at lower concentrations (e.g., 0.25%).
• Adjuvants:
Often combined with Dexamethasone, fentanyl, or epinephrine to enhance duration or onset.
Dosage and Administration
• Typical doses: o Peripheral nerve block: 10–40 mL of 0.25–0.5% (25–150 mg).
o Epidural: 10–20 mL of 0.25–0.5% (25–100 mg). o Spinal: 2–4 mL of 0.75% (15–30 mg).
• Maximum dose: 2–3 mg/kg (without epinephrine); 175 mg single dose, 400 mg/24 hr with epinephrine.
• Route: Perineural, epidural, intrathecal; not for IV use (high toxicity risk).
Safety Profile and Toxicity
• Systemic Toxicity (LAST - Local Aesthetic Systemic Toxicity):
o Cause: Accidental intravascular injection or overdose.
o Plasma threshold: ~4 µg/mL (toxic), >10 µg/mL (seizures).
o Symptoms: • CNS: Tinnitus, dizziness, seizures, coma.
• CVS: Bradycardia, hypotension, ventricular arrhythmias, cardiac arrest.
o Risk factors: High dose, rapid absorption, low protein binding in neonates/elderly.
• Cardiotoxicity:
o Mechanism: Blocks cardiac Nav and K+ channels, more pronounced than lidocaine.
o Outcome: Resistant ventricular arrhythmias, difficult resuscitation.
o Treatment: Lipid emulsion (20% IV), CPR, avoid vasopressin.
• Contraindications:
o Hypersensitivity to amides.
o IV regional anaesthesia (Bier block) due to toxicity risk.
o Severe hepatic impairment (reduced metabolism).
• Supraclavicular block:
o Bupivacaine 0.5%: Provides 4–8 hr analgesia alone.
o With Dexamethasone: Extends to 10–24 hr
Hemodynamic Stability:
Stable HR, SBP, DBP in study (e.g., 0 min: 74.33 bpm, 120.70/80.27 mmHg), consistent with Bupivacaine’s profile unless LAST occurs.
Pharmacology of Dexamethasone
General Overview
• Chemical class: Synthetic glucocorticoid (corticosteroid) [33-35]. \
• Chemical structure: 9-fluoro-11β,17,21-trihydroxy-16α- methylpregna-1,4-diene-3,20-dione.
• Formulations: Available as Dexamethasone base, sodium phosphate, or acetate; injectable forms (e.g., 4 mg/mL) used in nerve blocks.
Pharmacokinetics
• Absorption:
o Route: Oral, IV, IM, perineural (local adjuvant use).
o Rate: Rapid systemic absorption (IV/IM peak within 1 hr); local perineural absorption slower, site-dependent.
• Distribution:
o Volume of distribution (Vd): ~0.6–1 L/kg (wide tissue penetration).
• Metabolism:
o Site: Hepatic, via cytochrome P450 (CYP3A4).
o Pathways: Hydroxylation, conjugation to glucuronides/ sulphates.
• Excretion:
o Route: Primarily renal (~65% as metabolites, <10% unchanged).
o Half-life: 3–6 hours (biological half-life ~36–54 hours due to receptor effects).
o Clearance: ~0.1–0.2 L/h/kg (reduced in hepatic impairment).
Pharmacodynamics
• Mechanism of Action:
o oTarget: Glucocorticoid receptors (intracellular, cytosolic).
o oEffect: Binds receptors, translocates to nucleus, modulates gene expression.
o Primary actions:
• Anti-inflammatory:
Inhibits phospholipase A2, reduces prostaglandin/leukotriene synthesis.
• Immunosuppressive: Suppresses cytokine production (IL-1, IL-6, TNF-α).
• Membrane stabilization: Reduces neuronal excitability, enhances local anaesthetic effect.
• Onset of Action: o Systemic: 1–2 hours (IV/IM); peak effect 8–12 hours.
o Perineural: Immediate local effect (<30 min) when used as adjuvant, enhances block onset.
• Duration of Action:
o Systemic: 36–72 hours (long-acting due to receptor binding).
o Local (adjuvant): Prolongs nerve block by 8–24 hours (synergistic with Bupivacaine).
Clinical Uses
• Indications:
o Systemic: Allergic reactions, autoimmune diseases, cerebral oedema, inflammation.
o Local (adjuvant): Peripheral nerve blocks (e.g., supraclavicular), epidural/spinal anaesthesia.
• Role in nerve blocks:
o Dose: 4–8 mg (1–2 mL of 4 mg/mL solution) perineurally.
o Effect: Enhances onset, prolongs duration of local anaesthetics (e.g., Bupivacaine).
• Advantages:
o Extends analgesia (e.g., 10–24 hours with Bupivacaine vs. 4–8 hours alone).
o Reduces postoperative opioid need.
Dosage and Administration
• Systemic: o IV/IM: 0.5–9 mg/day (varies by condition).
• Local (adjuvant):
o Perineural: 4–8 mg (commonly 8 mg in studies).
o Route: Mixed with local anaesthetic (e.g., 23 mL Bupivacaine + 2 mL Dexamethasone).
• Maximum dose: No strict limit for single perineural use; systemic max ~20 mg/day.
Safety Profile and Toxicity
• Systemic Complication:
o Acute: Hyperglycaemia, hypertension, insomnia, mood changes.
o Chronic: Adrenal suppression, osteoporosis, Cushing’s syndrome (rare with single dose).
• Local (Perineural) Toxicity:
o oNeurotoxicity: Minimal in humans at 4–8 mg; animal studies suggest dose-dependent risk (>20 mg).
o Symptoms: Rare; transient paraesthesia reported, no permanent damage in clinical use
Clinical Relevance in Study Context
• Supraclavicular block: o Dose: 8 mg with 23 mL 0.5% Bupivacaine (Group D).
o Effect: Faster onset (e.g., sensory 3.93 ± 0.22 min vs. 5.20 ± 0.25 min in Group B), prolonged duration (inferred from hemodynamics).
• Mechanism in block:
o Local: Reduces perineural inflammation, stabilizes nerve membranes.
o Synergy: Enhances Bupivacaine’s sodium channel blockade.
• Hemodynamic stability:
No significant HR/BP changes (e.g., 30 min: 83.87 bpm, 130.70/89.27 mmHg), consistent with low systemic impact
Material and Method
This prospective, randomized observational, clinical study was conducted with 60 adult patients weighing between 60 to 80 kg in tertiary medical care hospital posted for elective upper limb surgeries having expected duration of surgery of 120 mins after taking written informed consent.
Study Duration: - June 2023-June 2025
• Patients were randomly divided into two groups of 30 patients each according to the local anaesthetic mixture they received by computer generated method.
• Group B (n=30) received Inj. 0.5% Bupivacaine 23 ml plus 0.9% normal saline 2 ml total volume of 25 ml.
• Group D (n=30) received 0.5% Bupivacaine 23 ml plus Dexamethasone 2 ml (8 mg). total volume of 25 ml.
The Inclusion Criteria were
• Patients aged between 18 and 60 years
• Patients with ASA I & II physical status
• Patients who were planned to undergo lower arm, elbow and forearm Surgeries only elective under supraclavicular brachial plexus block.
The Exclusion Criteria were
• Patient’s refusal
• Pregnant women
• History of local anaesthetics allergy
• Peripheral neuropathy
• Patient with psychiatric behaviours
• Bleeding disorder
• Patients on anticoagulants
• Neurological deficit involving brachial plexus
• Local infection at the injection site.
Pre-Operative Assessment
All the patients were assessed thoroughly preoperatively. Any significant past, family, personal history was taken. General and systemic examination were done. Vitals (HR, BP, Spo2) and investigations were noted. Detailed airway examination was done. Patients were kept NBM for 6 hrs prior to surgery.
• After explaining the procedure properly, a written informed consent was taken from all the patients of the study.
• Each patient was explained in detail regarding the procedure of anaesthesia and VISUAL ANALOGUE SCALE (VAS) was explained on a sheet of paper where a score of 0 labelled as no pain and 10 as worst possible pain.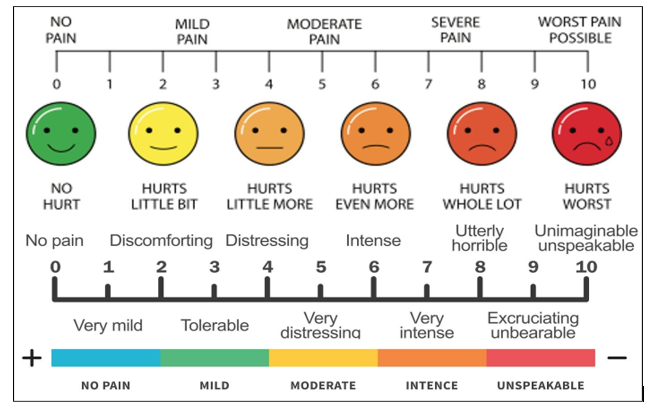
Pre-Operative Preparation
OT Preparation
• Anaesthesia machine with working l a r y n g o s c o p e , airway, endotracheal tubes, face mask and Bain’s circuit.
Drugs required for: Conventional general anaesthesia Resuscitation
• Suction machine
• Multipara monitor
• USG machine
• ECG electrode
• A sterile tray containing
o Disposable 10cc syringe,
o Disposable 23G 1.5-inch block needle,
o Disposable syringe with 25G 1-inch needle filled with lignocaine (2%) 2ml for local infiltration,
o Sterile swab holding forceps,
o Adequate cotton swabs,
o Antiseptic solution o Sterile towel
Drug Preparation
• Local anaesthetic solution: Sterile vial containing - Inj. Bupivacaine Hydrochloride 0.5% - 2ml
• Inj. Dexamethasone: sterile preservative free 2 ml ampoule containing 8 mg:
|
Group |
Dose |
|
B |
Inj. Bupivacaine 0.5% 23ml + Inj. NS 0.9% 2ml |
|
D |
Inj. Bupivacaine 0.5% 23ml + Inj. Dexamethasone 2ml |
Patient Preparation
The patient was kept nil by mouth for 6 hours before surgery. In the operating theatre, multipara monitor attached and vitals (baseline heart rate, blood pressure, respiratory rate, and SpO2) recorded. IV line was set up with Ringer's Lactate, and the procedure was explained to the patient.
Anesthetic Technique
• On the operation table, the patient was given the position for brachial plexus block via supraclavicular approach. In supine position with the patient’s head turned away from the side to be blocked. The arm to be anaesthetized is adducted and the hand extended along the side towards the ipsilateral knee as far as possible. Under all aseptic and antiseptic precaution local site was painted and draped.
• We used an Ultrasound machine with linear transducer for localization of the brachial plexus. The transducer is positioned in the transverse plane immediately proximal to the clavicle, slightly posterior to its midpoint. The transducer is tilted caudally, to obtain a cross-sectional view of the subclavian artery. The brachial plexus is seen as a collection of hypoechoic oval structures posterior and superficial to the artery.
The 23-gauge 1.5inch block needle was then inserted in plane toward the brachial plexus, in a lateral to medial direction. Upon visualizing the needle path to the desired location, the study local anaesthetic mixture was injected after negative aspiration for blood and air.
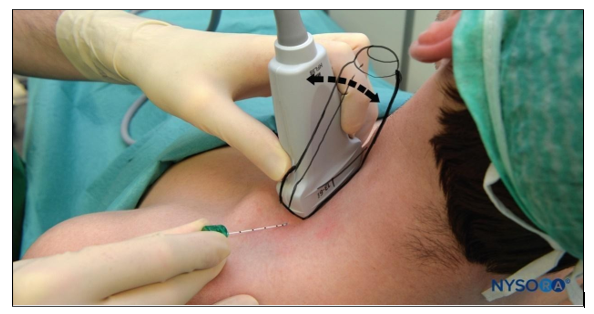
Figure 1: Supraclavicular Brachial Plexus: Transducer Position & Needle Insertion
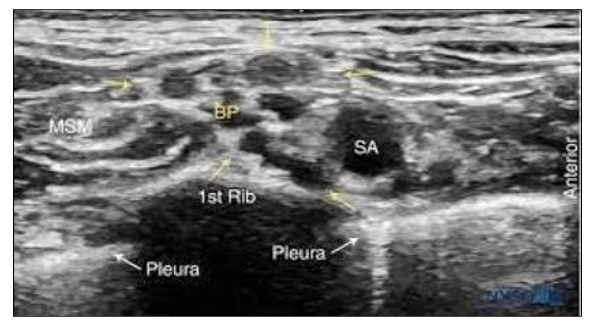
Figure 2: Ultrasound Image of the Brachial Plexus (BP) Assuming an Oval Shape and Circled by the Tissue Sheath (Yellow Arrows)
• During the conduct of the block and thereafter, the patients were observed vigilantly for any procedure related complications and for the toxicity of the drugs injected. After injection of the local anaesthetic, the following parameters were studied:
Onset of Sensory Block
That was assessed using the blunt end of a needle by pin prick method along the course of major peripheral nerves (ulnar, radial, medial and musculocutaneous). Sensory block was graded according to the following scale:
• Grade 0 = no block (normal sensation)
• Grade 1 = partial block (decreased sensation)
• Grade 2 = complete block (no sensation)
Onset of Sensory Blockade was taken as time from end of injection of LA drug to feeling of decreased sensation and numbness (grade 1) in areas of nerve to be assessed.
Peak (Complete) of Sensory Blockade was taken as the time from the end of injection of LA drug to complete loss of pin prick sensation (grade 2) in areas of nerve to be assessed.
Onset of Motor Block
Motor block characteristics were measured by assessing the following motor functions:
i. Flexion of the elbow (musculocutaneous nerve),
ii. Extension of the elbow and the wrist (radial nerve),
iii. Opposition of the thumb and index finger (median nerve),
iv. Opposition of the thumb and small finger (ulnar nerve). Motor block was graded according to the following scale:
• Grade 0 = no block (full muscle activity)
• Grade 1 = partial block (decreased muscle activity)
• Grade 2 = complete block (no muscle activity).
Onset of Motor Blockade was taken as time from end of injection of LA drug to decreased muscle activity (grade 1).
Peak (Complete) of Motor Blockade was defined as the time from the end of injection of LA drug to no muscle activity (grade 2).
Only patients with complete motor and sensory block were included in the study.
After achieving complete motor and sensory block, surgery was allowed to start and time of starting of surgery was noted.
Hemodynamic Vitals (heart rate, blood pressure, respiratory rate, SpO2) were recorded at 1,5,10,15,30 every 15 mins till the end of surgery from the end of injection of local anaesthetic. Intravenous fluids were continued in the intraoperative period at a rate of 2ml/ kg/hour.
Intraoperative Complications like hypotension (fall in mean arterial blood pressure >20% from baseline), hypertension, Bradycardia (Heart rate < 60/min), tachycardia, breathlessness, shivering, nausea and vomiting were observed.
Total duration of each surgery (from incision to end of surgery) was noted.
Post-Operative Follow-up was carried out in the recovery and postoperative ward. Hemodynamic vitals (heart rate, blood pressure, respiratory rate, SpO2) and any complication were noted. VAS score for pain was evaluated till the need for the 1st rescue analgesia needed and in between whenever patient complained of pain.
Duration of Motor Block was defined as the time elapse between the onset motor blockade to return of motor power evaluated by finger movement.
Duration of Sensory Block was defined as time elapse between onset of sensory blockade to return of pin prick sensation.
Time for Rescue Analgesia (Min) was defined as time duration between the onset of sensory blockade to when patient experiencing the pain of VAS ≥ 4 severity. When the patients began to experience pain (VAS ≥ 4), it was considered that analgesic action of the drugs was terminated and rescue analgesic in the form of injection Diclofenac 1-1.5mg/kg iv was given.
Results were statistically analysed by independent student’s t-test and results were expressed as mean ± SD.
We used Microsoft Excel 2007 version software.
|
“p” value > 0.05 |
Statistically non-significant |
|
“p” value < 0.05 |
Statistically significant |
|
“p” value <0.001 |
Statistically highly significant |
Proforma
Comparison of Dexamethasone with Bupivacaine and Bupivacaine Alone in Supraclavicular Brachial Plexus Block for Post-Operative Analgesia.
Patient Data:
Name: Date:
Age/sex: Indoor reg no:
Diagnosis: ASA grade:
Type of surgery:
Pre-operative Assessment:
Present complain:
Past medical history:
Previous operative and anaesthesia history:
H/o drug allergy/addiction/blood transfusion:
H/o any bleeding disorder:
Family history:
Personal history:
Obstetric history:
General Examination:
Level of consciousness:
Weight:
Height:
Pallor: Oedema:
Clubbing: Cyanosis:
Icterus:
Vital Data
Temperature:
Heart rate:
Blood pressure:
Spo2(oxygen saturation):
Systemic Examination:
RS:
CVS:
CNS:
P/A:
Others:
Airway Examination: Breath holding time:
Mouth opening: Mallampati grade:
Neck movement: Teeth:
Local Examination of Supraclavicular Area
Infection: Swelling:
Trauma: Deformity:
Investigations:
Complete Hemogram:
RBS: Electrolyte:
RFT: LFT:
PT/INR:
CXR (PA view):
ECG: HIV, HbsAg:
Others as and when required:
NBM hours:
Premedication:
Inj Glycopyrrolate 0.2 mg Intravenously
Inj Ondansetron 4 mg Intravenously
Monitoring:
Heart rate, ECG, BP, Respiratory Rate, SpO2
Details of Procedure:
Position: Supine position, with head turned to opposite side Side: Right / Left
Approach: Supraclavicular brachial plexus block
Needle: 23 Gauge 1.5inch block needle
Method of localization: USG guided
Local Anaesthetic:
Group B: Inj.23 ml 0.5% Bupivacaine +2 ml 0.9% normal saline
Group D: Inj.23ml 0.5% Bupivacaine +2 ml Dexamethasone (8 mg)
Time of onset of sensory block:
Time of onset of motor block:
Time to achieve peak sensory block:
Time to achieve peak motor block:
Duration of Surgery:
Peri Operative Monitoring:
|
Time |
Heart rate |
SBP |
DBP |
SPO2 |
complication |
|
Pre-operative |
|
|
|
|
|
|
1 min |
|
|
|
|
|
|
5 min |
|
|
|
|
|
|
10 min |
|
|
|
|
|
|
15 min |
|
|
|
|
|
|
30 min |
|
|
|
|
|
|
45 min |
|
|
|
|
|
|
60 min |
|
|
|
|
|
|
75 min |
|
|
|
|
|
|
90 min |
|
|
|
|
|
|
120 min |
|
|
|
|
|
|
POST OP |
||||||
|
Time |
Heart rate |
SBP |
DBP |
SPO2 |
VAS SCORE |
Complication |
|
Immediate post op |
|
|
|
|
|
|
|
1 hr |
|
|
|
|
|
|
|
3 hr |
|
|
|
|
|
|
|
5 hr |
|
|
|
|
|
|
|
7 hr |
|
|
|
|
|
|
|
9 hr |
|
|
|
|
|
|
|
12 hr |
|
|
|
|
|
|
|
18 hr |
|
|
|
|
|
|
Complication:
Intraoperative
Tachycardia/bradycardia
Breathlessness
Shivering
Hypotension/hypertension
Nausea & vomiting
Others
Postoperative
Hematoma
Pneumothorax
ausea/vomiting
Hypotension/hypertension
Bradycardia/tachycardia
Post-Operative Observation:
Duration of motor blockade recovery mins
Duration of sensory blockade recovery mins
Time to requirement of 1st rescue analgesia (VAS≥4) -------mins.
Observation and Results
After studying 60 cases, the observations and results are summarized in tabulated form and are described below. Each group contains 30 patients.
|
Parameters |
Group D (Mean±SD) |
Group B (Mean±SD) |
p Value |
Inference |
|
Age (Years) |
36.07 ± 9.93 |
37.47 ±10.02 |
0.59 |
NS |
|
Weight (Kg) |
66.27 ± 6.56 |
65.57 ± 6.77 |
0.69 |
NS |
|
Sex(M/F) |
18:12 |
19:11 |
0.79 |
NS |
|
ASA Grade I&II |
22&8 |
24&6 |
0.54 |
NS |
Table 1: Demographic Data
The demographic and clinical parameters (age, weight, sex, ASA status) of Group D and Group B are statistically similar (p > 0.05), ensuring comparability. This homogeneity supports attributing postoperative analgesia differences primarily to Dexamethasone rather than confounding variables.
|
Parameters |
Group D (Mean±SD) |
Group B (Mean±SD) |
p Value |
Inference |
|
Onset of Sensory Block (min) |
3.93 ±0.22 |
5.20 ± 0.21 |
<0.0001* |
S |
|
Onset of Motor Block (min) |
5.52 ±0.21 |
6.67 ± 0.23 |
0.0001* |
S |
Table 2: Onset of Sensory and Motor Block
The table shows that Group D achieves significantly faster onset of sensory (3.93 min) and motor (5.52 min) blocks compared to Group B (5.20 min and 6.67 min), with p-values of 0.0001. This indicates that Dexamethasone markedly accelerates the initial establishment of both sensory and motor blockade.
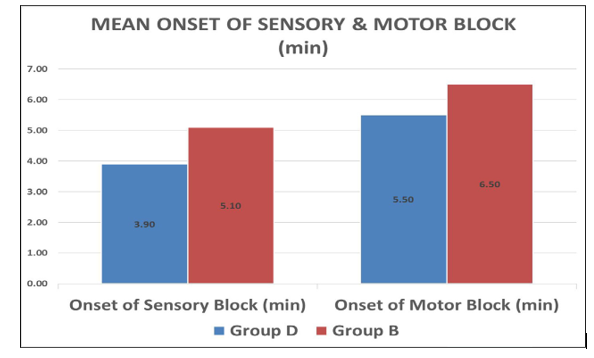
Graph 1: Showing Mean Sensory and Motor Block of Group B and Group D
|
Intraop changes in HEART RATE PER MIN |
||||
|
PR |
Group D |
Group B |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
PRE-OP |
85.00 |
4.45 |
85.80 |
3.84 |
|
1 min |
91.40 |
3.68 |
90.80 |
2.61 |
|
5 min |
91.60 |
4.01 |
92.53 |
4.61 |
|
10 min |
89.73 |
5.22 |
89.60 |
3.34 |
|
15 min |
86.13 |
5.17 |
86.13 |
3.23 |
|
30 min |
80.80 |
5.24 |
81.00 |
4.03 |
|
45 min |
79.80 |
5.07 |
80.20 |
4.37 |
|
60 min |
80.47 |
4.89 |
80.73 |
4.08 |
|
75 min |
79.47 |
5.28 |
79.67 |
3.68 |
|
90 min |
79.67 |
4.87 |
81.40 |
4.27 |
|
120 min |
80.53 |
4.90 |
80.67 |
4.50 |
|
Postop changes in HEART RATE PER HR |
||||
|
PR |
Group D |
Group B |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
Immediate post op |
81.60 |
5.05 |
83.40 |
4.27 |
|
Post op 1 hr |
83.20 |
5.35 |
83.73 |
5.09 |
|
Post op 3 hr |
82.20 |
5.59 |
84.27 |
5.63 |
|
Post op 5 hr |
83.80 |
5.21 |
84.87 |
4.45 |
|
Post op 7 hr |
83.27 |
5.32 |
84.93 |
3.96 |
|
Post op 9 hr |
84.40 |
5.21 |
86.00 |
4.03 |
|
Post op 12 hr |
85.27 |
5.39 |
87.07 |
3.10 |
|
Post op 18 hr |
85.07 |
4.32 |
86.00 |
3.64 |
Table 3: Intraop and Post Op Changes in Heart Rate
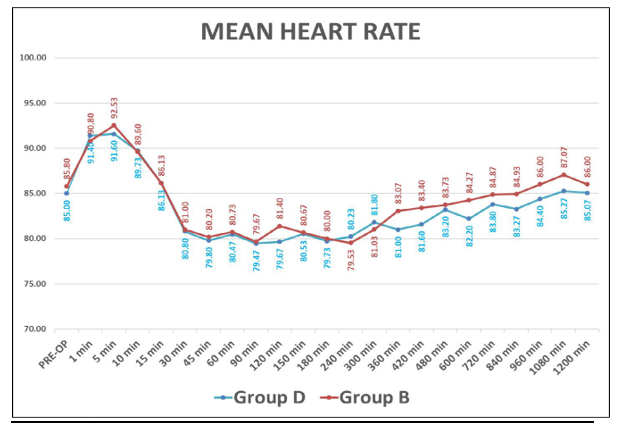
Graph 2: Showing Intraop And Postop Changes in Mean Heart Rate
|
SBP |
Group D |
Group B |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
PRE-OP |
124.53 |
6.89 |
125.20 |
7.17 |
|
1 min |
126.20 |
6.87 |
126.67 |
8.26 |
|
5 min |
124.07 |
7.99 |
124.47 |
5.14 |
|
10 min |
122.17 |
8.28 |
123.00 |
6.47 |
|
15 min |
120.53 |
7.74 |
121.27 |
6.31 |
|
30 min |
119.47 |
7.52 |
121.47 |
7.48 |
|
45 min |
119.07 |
6.96 |
121.73 |
7.20 |
|
60 min |
118.40 |
5.67 |
118.07 |
5.79 |
|
75 min |
119.67 |
6.13 |
119.07 |
5.86 |
|
90 min |
119.60 |
6.42 |
118.27 |
5.77 |
|
120 min |
119.20 |
5.19 |
118.27 |
5.82 |
|
Postop changes in SBP (mmHg) |
||||
|
SBP |
Group D |
Group B |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
Immediate post op |
120.07 |
5.72 |
118.40 |
5.29 |
|
Post op 1 hr |
119.67 |
6.13 |
119.07 |
5.86 |
|
post op 3 hr |
122.93 |
6.82 |
120.87 |
7.31 |
|
post op 5 hr |
123.20 |
7.46 |
120.47 |
4.60 |
|
post op 7 hr |
119.67 |
6.06 |
119.07 |
6.16 |
|
post op 9 hr |
121.40 |
6.63 |
120.60 |
7.07 |
|
post op 12 hr |
120.47 |
7.59 |
118.87 |
6.07 |
|
post op 18 hr |
120.73 |
6.25 |
121.20 |
7.27 |
Table 4: Intraop Changes in SBP (mmHg)
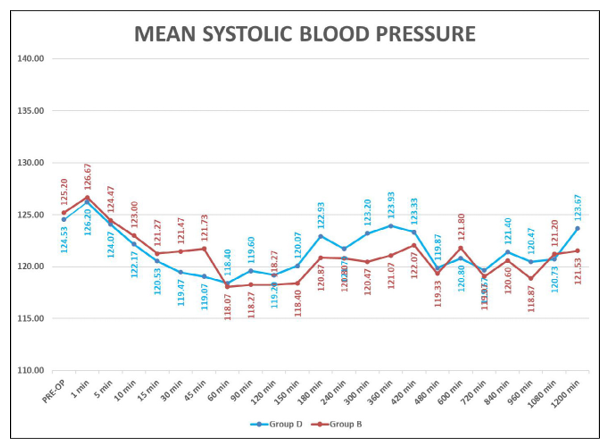
Graph 3: Showing Mean Systolic Blood Pressure (mmHg)
|
DBP |
Group D |
Group B |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
PRE-OP |
79.60 |
5.29 |
80.07 |
5.37 |
|
1 min |
78.53 |
4.39 |
78.20 |
5.05 |
|
5 min |
77.60 |
6.07 |
78.13 |
5.48 |
|
10 min |
77.27 |
5.05 |
77.67 |
5.44 |
|
15 min |
77.07 |
4.35 |
77.27 |
4.80 |
|
30 min |
78.60 |
3.45 |
78.27 |
5.27 |
|
45 min |
78.13 |
4.10 |
76.27 |
5.98 |
|
60 min |
79.33 |
3.94 |
77.60 |
4.88 |
|
75 min |
78.93 |
3.91 |
78.27 |
4.76 |
|
90 min |
80.53 |
4.17 |
78.27 |
5.25 |
|
120 min |
80.33 |
4.14 |
78.20 |
5.26 |
|
POSTOP CAHNGES IN DBP (mmHg) |
||||
|
DBP |
Group D |
Group B |
||
|
MEAN |
SD |
MEAN |
SD |
|
|
immediate post op |
80.73 |
4.44 |
79.07 |
3.67 |
|
Post op 1 hr |
78.93 |
3.91 |
78.27 |
4.76 |
|
post op 3 hr |
78.93 |
3.78 |
77.73 |
5.32 |
|
post op 5 hr |
79.80 |
3.73 |
78.27 |
5.30 |
|
post op 7 hr |
80.67 |
3.61 |
79.20 |
4.38 |
|
post op 9 hr |
81.67 |
3.90 |
79.87 |
4.52 |
|
post op 12 hr |
78.93 |
4.45 |
78.60 |
6.39 |
|
post op 18 hr |
80.60 |
3.72 |
78.33 |
5.97 |
Table 5: Intraop changes in DBP (mmHg)
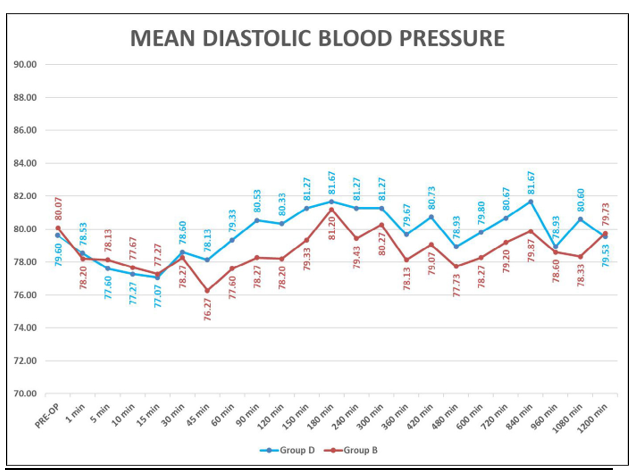
Graph 4: Showing Mean Diastolic Blood Pressure (Mmhg)
This table shows perioperative heart rate and blood pressure (Systolic and Diastolic blood pressure) in patients. There was no significant difference in mean heart rate of patients of both the group(P>0.05) and heart rate blood pressure were stable and comparable between two groups.
|
TIME (MIN) (intraop) |
RESPIRATORY RATE (PER MIN) |
SPO2 (%) |
||
|
Group D |
Group B |
Group D |
Group B |
|
|
MEAN±SD |
MEAN±SD |
MEAN±SD |
MEAN±SD |
|
|
PRE-OP |
16.50±1.22 |
16.03±1.13 |
98.80±0.41 |
98.83±0.38 |
|
1 min after injection of LA |
17.33±0.99 |
17.13±1.11 |
98.93±0.25 |
98.97±0.18 |
|
5 min |
17.57±0.73 |
17.60±0.77 |
98.87±0.35 |
98.93±0.25 |
|
10 min |
17.00±1.23 |
17.07±1.20 |
98.93±0.45 |
99.00±0.37 |
|
15 min |
16.67±1.32 |
16.77±1.38 |
99.00±0.00 |
98.97±0.32 |
|
30 min |
16.63±1.35 |
16.73±1.41 |
99.00±0.00 |
98.97±0.18 |
|
45 min |
16.67±1.32 |
16.77±1.38 |
99.00±0.00 |
99.00±0.00 |
|
60 min |
16.63±1.35 |
16.73±1.41 |
99.00±0.00 |
99.00±0.00 |
|
90 min |
16.80±1.21 |
16.73±1.36 |
99.00±0.00 |
99.00±0.00 |
|
120 min |
16.60±1.38 |
16.57±1.38 |
99.00±0.00 |
99.00±0.00 |
Table 6: Intraop and post op changes in
Respiratory Rate And Spo2 Changes
|
TIME (MIN) (post op) |
RESPIRATORY RATE (PER MIN) |
SPO2 (IN %) |
||
|
Group D |
Group B |
Group D |
Group B |
|
|
MEAN±SD |
MEAN±SD |
MEAN±SD |
MEAN±SD |
|
|
Immediate post op |
16.63±1.35 |
16.73±1.41 |
99.00±0.00 |
99.00±0.00 |
|
Post op 1 hr |
16.63±1.35 |
16.73±1.41 |
99.00±0.00 |
98.97±0.18 |
|
Post op 5 hr |
16.63±1.35 |
16.73±1.41 |
99.00±0.00 |
99.00±0.00 |
|
Post op 7 hr |
16.63±1.35 |
16.73±1.41 |
99.00±0.00 |
99.00±0.00 |
|
Post op 9 hr |
16.67±1.37 |
16.73±1.41 |
99.00±0.00 |
99.00±0.00 |
|
Post op 12 hr |
16.67±1.21 |
16.70±1.26 |
99.00±0.00 |
99.00±0.00 |
|
Post op 18 hr |
16.53±1.36 |
16.57±1.41 |
99.00±0.00 |
99.00±0.00 |
Post op changes in RR & spo2
This table shows mean respiratory rate and spo2(Oxygen saturation) of patients in perioperative period. There was no significant difference in mean respiratory rate and spo2 of patients of both the groups(P>0.05), respiratory rate and spo2 were stable and comparable between two groups.
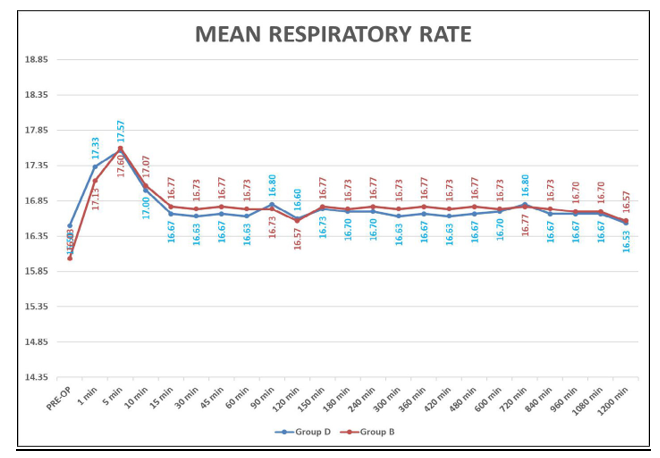
Graph 5: Showing Mean Respiratory Rate
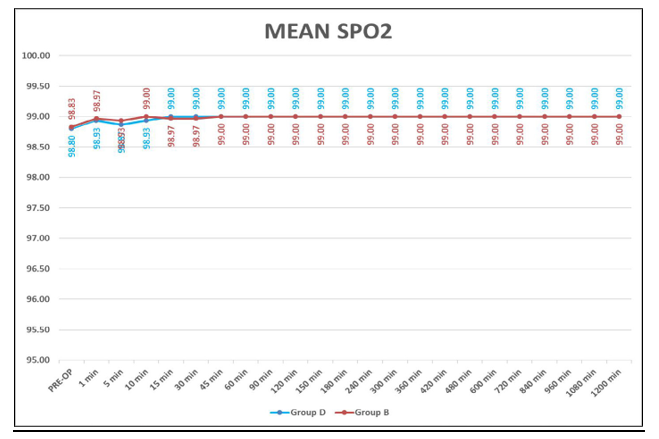
Graph 6: Showing Mean Spo2(%)
|
Parameters |
Group D (Mean±SD) |
Group B (Mean±SD) |
p Value |
Inference |
|
Peak of Sensory Block (min) |
9.40 ± 0.93 |
11.50 ± 0.78 |
<0.0001* |
S |
|
Peak of Motor Block (min) |
12.30 ± 1.32 |
15.87 ± 1.17 |
<0.0001* |
S |
Tbale 7: Peak Of Sensory And Motor Block
This table shows mean time to achieve peak (complete) sensory and motor block.
The time to achieve peak (complete) sensory and motor blockade were significantly more rapid in the Group D than in the Group B (P<0.05).
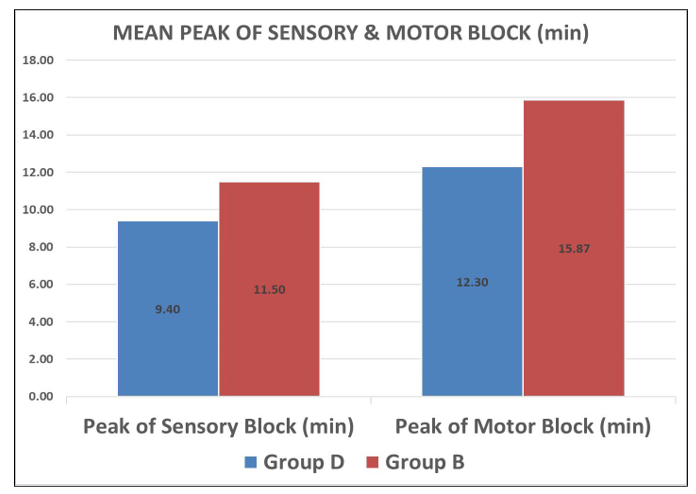
Graph 7: Showing Mean Peak of Sensory and Motor Block
|
Parameters |
Group D (Mean±SD) |
Group B (Mean±SD) |
P value |
inference |
|
Duration of Motor Block (min) |
598.17 ± 28.05 |
460 ± 22.89 |
<0.0001 |
S |
|
Duration of sensory block (min) |
807.50±24.45 |
510±17.8 |
<0.0001 |
S |
Table 8: Duration Of Motor & Sensory Block
Group D (with Dexamethasone) significantly extends the duration of motor block (598.17 ± 28.05 min vs. 460 ± 22.89 min in Group B) and sensory block (807.50±24.45 min vs. 510±17.8min), both with p < 0.0001, indicating enhanced block duration.
|
Parameters |
Group D (Mean±SD) |
Group B (Mean±SD) |
P value |
inference |
|
Time to first rescue Analgesia (min) |
1010 ± 40.66 |
580 ± 24.91 |
<0.0001* |
S |
Table 9: Time To First Rescue Analgesia
The table shows a significant difference in time to first rescue analgesia between the two groups. Group D (with dexamethasone) had a longer duration (1010 ± 40.66 min) than Group B (bupivacaine alone, 580 ± 24.91 min), with P < 0.0001. This indicates that dexamethasone significantly prolongs postoperative analgesia when used with bupivacaine.
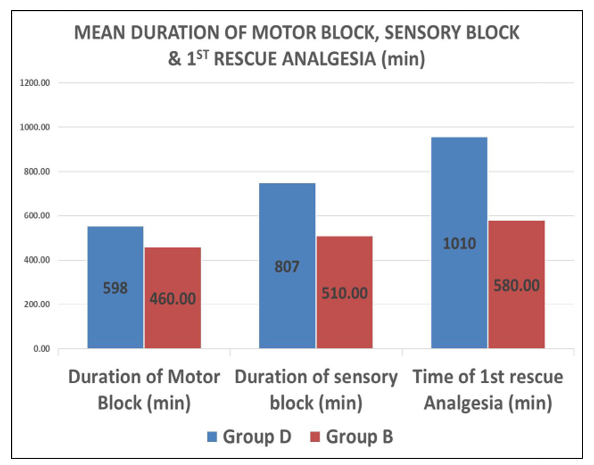
Graph 8: Showing Duration of Sensory & Motor Block and 1st Rescue Analgesia
|
Parameters |
Group D (Mean±SD) |
Group B (Mean±SD) |
p Value |
Inference |
|
Duration of Surgery (min) |
110.17 ± 20.28 |
108 ± 17.30 |
0.66 |
NS |
Table 10: Duration of Surgery
This table shows Duration of surgery in both the groups were comparable and there was no statically significant difference(p>0.05)
Graph 9: Showing the Mean Duration of Surgery
|
Complication |
Group D (N=30) |
Group B (N=30) |
|
INTRAOPERATIVE |
||
|
Tachycardia/Bradycardia |
0 |
0 |
|
Hypotension/Hypertension |
0 |
0 |
|
Breathlessness |
0 |
0 |
|
Nausea/vomiting |
0 |
1 |
|
Shivering |
0 |
1 |
|
Others |
0 |
0 |
|
Complication |
Group D (N=30) |
Group B (N=30) |
|
POST OPERAATIVE |
||
|
Hematoma |
0 |
0 |
|
Neurological sequalae |
0 |
0 |
|
Pneumothorax |
0 |
0 |
|
Surgical emphysema |
0 |
0 |
|
Nausea/vomiting |
0 |
1 |
|
Hypotension/hypertension |
0 |
0 |
|
Shivering |
0 |
2 |
Table 11: Perioperative Complication (Any)
Any complications related to drugs and procedure, hemodynamic and neurological complications were not seen in either of the groups. Only one patient from Group B had nausea during intraoperatively which was managed by Inj. Ondansetron 4 mg IV. Only two patients from Group B had shivering in post operative period for which no pharmacological interventions were required, only treated with warm blanket.
|
VISUAL ANALOGUE SCALE |
Group D |
Group B |
p VALUE |
||
|
Frequency |
% |
Frequency |
|||
|
Immediate Post op |
0 |
17 |
57% |
0 |
<0.0001 |
|
|
1 |
13 |
43% |
11 |
|
|
|
2 |
0 |
0% |
19 |
|
|
1 hr |
0 |
9 |
30% |
0 |
<0.0001 |
|
|
1 |
21 |
70% |
0 |
|
|
|
2 |
0 |
0% |
21 |
|
|
|
3 |
0 |
0% |
9 |
|
|
3 hr |
1 |
16 |
53% |
0 |
<0.0001 |
|
|
2 |
14 |
47% |
11 |
|
|
|
3 |
0 |
0% |
19 |
|
|
5 hr |
1 |
9 |
30% |
0 |
<0.0001 |
|
|
2 |
21 |
70% |
0 |
|
|
|
3 |
0 |
0% |
20 |
|
|
|
4 |
0 |
0% |
10 |
|
|
7 hr |
2 |
18 |
60% |
12 |
0.0497 |
|
|
3 |
12 |
40% |
9 |
|
|
|
4 |
0 |
0% |
8 |
|
|
|
5 |
0 |
0% |
0 |
|
|
9 hr |
2 |
13 |
43% |
2 |
0.0001 |
|
|
3 |
17 |
57% |
9 |
|
|
|
4 |
0 |
0% |
15 |
|
|
|
5 |
0 |
0% |
4 |
|
|
12 hr |
2 |
0 |
0% |
0 |
0.0006 |
|
|
3 |
17 |
57% |
2 |
|
|
|
4 |
13 |
43% |
14 |
|
|
|
5 |
0 |
0% |
11 |
|
|
|
6 |
0 |
0% |
3 |
|
|
18 hr |
3 |
0 |
0% |
1 |
0.0006 |
|
|
4 |
24 |
80% |
14 |
|
|
|
5 |
6 |
20% |
12 |
|
|
|
6 |
0 |
0% |
3 |
|
Table 12: Post Operative Vas Score
All time points show significant differences (p < 0.05), with p-values ranging from <0.0001 to 0.0497, indicating that Group D has lower VAS scores (better pain control) compared to Group B across the postoperative period. This supports Dexamethasone’s post operative analgesic effect.
Discussion
Brachial plexus block acts as sole anaesthetic technique to provide painless upper limb surgery. Many approaches have been mentioned of which the classical supraclavicular approach is most common to brachial plexus for the whole upper limb surgeries because of compact arrangement of the nerve trunks. By adding various adjuvants, it blocks all branches of brachial plexus.
For less drug requirement, less complication and more accuracy, we have chosen USG guided Supraclavicular brachial plexus block. USG guided technique not only enables to secure an accurate needle position but one can also monitor the distribution of the local anaesthetic in real time, with the potential advantage of improving the quality of nerve block, shortening the latency of the block, and reducing the minimum volume required to obtain a successful nerve block [1,3,8,17].
Management of pain in postoperative cases reduces suffering especially in orthopaedic surgeries and give early mobilization, brief hospital stays, reduction in hospitalization and greater patient satisfaction. Brachial plexus block technique provides best alternative to General anaesthesia [14].
Dexamethasone, long acting and highly potent glucocorticoid has desirable properties of stable hemodynamic, no sedation, no respiratory depression, along with potentiating and prolonging the duration of analgesia through its (i) vasoconstrictive effect there by reducing the local anaesthetics absorption and (ii) increasing the activity of inhibitory potassium channels on nociceptive C-fibres (via glucocorticoid receptors), thus decreasing their activity without any unwanted complication.
The present study was performed to compare the efficiency of Dexamethasone when administered with a mixture of 0.5% Bupivacaine in USG guided supraclavicular approach of brachial plexus blockade on post-operative analgesia. Onset, peak effect of sensory and motor blockade, duration of sensory and motor blockade and time of 1st rescue analgesia as well as peri-operative hemodynamic changes and complication were also studied.
Demographic Data
Demographic data in term of age, sex, weight and ASA status of patients were comparable in both groups of study.
Duration of Surgery
The mean duration of surgery was comparable in both groups in our study.
The mean duration of surgery was 108 ± 17.30 mins in Group B and 110.17 ± 20.28 mins in Group D.(P>0.05)
Onset of Sensory and Motor Block
The mean onset of sensory blockade in Group D(Dexamethasone) was 3.90 ± 0.84 mins as compared to 5.10 ± 0.92 mins in Group B and the mean onset of motor blocked in Group D was 5.50 ± 1.04 mins as compared to 6.5 ± 0.82 mins in Group B. In our study, the time of onset of sensory and motor block was significantly faster in Dexamethasone group(p<0.05).
In our study, in both the groups the onset of sensory block was earlier than motor blockade. Our results correlate with the finding of other study with earlier onset of sensory block than motor block [21].
M.P. Golwala et al. concluded that addition of Dexamethasone in their study the mean time of onset of sensory block in control group was 275.66 ± 30.32 sec and in Dexamethasone receiving group was 196.33 ± 26.45 sec [36]. The mean time of Onset of motor block in control group was 326.66 ± 27.20 sec and in Dexamethasone receiving group was 225.66 ± 26.86 sec.
Nilesh M. Solanki et al. reported that mean onset time of sensory block was 4.24 ± 1.42 min in control group and 3.24 ± 1.09 min in Dexamethasone group [37]. The mean onset time of motor block was 7.52 ± 1.50 min in control group and 6.2 ± 1.44 min in Dexamethasone group. The difference was statistically significant(p<0.05).
Peak Effect of Sensory & Motor Blockade
In our study, the mean time to achieve peak of sensory block in Group B was 11.50 ± 0.78 min and Group D was 9.40 ± 0.93 min. The mean time to achieve peak of motor block in Group B was 15.87 ± 1.17 min and Group D was 12.30 ± 1.32 min.
The time to achieve peak sensory block and motor block was significantly faster in Dexamethasone group compared with Bupivacaine group (p< 0.05).
Ramakrishna shatagopam et al. concluded that mean duration of peak of sensory blockade in control group was 17.4 ± 3.5 min and in Dexamethasone group was found to be 11.8 ± 2.7 min and the mean duration of peak of motor blockade in control group was 8.5 ± 4.4 min and in Dexamethasone group was found to be 6.4 ±1.8 min [38].
Shwetank Rai et al. had conducted that mean duration of peak of sensory blockade in control group was 8.43 ± 1.04 min and in Dexamethasone group was found to be 6.49 ± 1.09 min and the mean duration of peak of motor blockade in control group was 17.53 ± 1.70 min and in Dexamethasone group was found to be 14.63 ± 2.79 min [39].
M.P. Golwala et al. concluded that addition of Dexamethasone in their study the mean peak effect time of sensory and motor block was 708.33 ± 50.58 sec and 767.33 ± 47.26 sec in control group and 544.33 ± 47.68 sec and 651.33 ± 38.75 sec in Dexamethasone receiving group respectively [36]. The mean time of peak of sensory block and motor block was significantly faster in Dexamethasone group and statistically significant (p < 0.05).
Duration of Motor Block, Sensory Block and Time of 1st Rescue Analgesia
In our study, the mean time of duration of motor block, mean time of duration of sensory block and mean time for 1st rescue analgesia in Group B was 460 ± 22.89 min, 510±17.86 min & 622.66 ± 32.34 min and in Group D was 580 ± 24.91 min, 807.5±24.45 min & 1010 ± 40.66 min respectively.
We found a statistically significant difference in duration of motor and sensory block and time of 1st rescue analgesia between both the groups(p<0.05).
We observed that adding Dexamethasone to plain Bupivacaine (0.5%) significantly prolongs the effect of motor and sensory block and also delays the time for the need of rescue analgesia in supraclavicular block.
Ramakrishna shatagopam et al. found that mean duration of sensory blockade in was 2.3 ± 1.4 hours in normal Bupivacaine group and was found to be 5.85 ± 0.84 hours in Dexamethasone group and the mean duration of motor blockade was 2.48 ± 0.59 hours in normal Bupivacaine group and was found to be 6.97 ± 0.47 hours in Dexamethasone group [38].
Khalid ali Khaleel et al. concluded that mean duration of se was found to be 289.50 ± 45.71 min in normal Bupivacaine group and the mean duration of motor blockade was 870.87 ± 101.14 min in Dexamethasone group and was found to be 216.27 ± 37.73 min in normal Bupivacaine group and was highly statistically significant [40].
Nilesh M. Solanki et al. concluded that the duration of motor block was prolonged in Dexamethasone group (463.2±35.20 min) as compared to control group(251.4±18.68min) [37]. The difference was statistically significant(p<0.05). There was markedly prolonged duration of analgesia in Dexamethasone group ,12-16hr (mean 855.6±83.81min) compared to control group, 4-5hr (mean 276.16±20.44min).
M.P. Golwala et al. concluded that addition of Dexamethasone produces prolongation postoperative analgesia 12-18 hours as compared to 4-6 hours in control group [36].
Perioperative Hemodynamic
In our study, there was no significant difference in the hemodynamic found between the two groups perioperatively. During intraoperative period, hemodynamic remained stable in consistent manner, thereby reducing any anxiety related fluctuations in the vitals.
M.P. Golwala et al. demonstrated in their study that, no significant difference in both group of study in terms of hemodynamic variables like heart, blood pressure, Spo2 [36].
Shreshta B.R. et al. concluded that hemodynamics remained stable in both groups intraoperatively and postoperatively [17].
Perioperative Complications
Only one patient from Group B had nausea during intraoperatively which was managed by Inj. Ondansetron 4 mg IV. Only two patients from Group B had shivering in post operative period for which no pharmacological interventions were required only treated with warm blanket
M.P. Golwala et al. showed in their study that no adverse effects were occurred in Dexamethasone group and control group intraoperatively and postoperatively [36].
Shreshta B.R. et al. used Dexamethasone and demonstrated that there were no adverse effects like nausea, vomiting, bradycardia, hypotension was occurred in either group intraoperatively and postoperatively [17].
Summary and Conclusion
After taking thorough history and pre-operative assessment and Informed consent, a comparative study of 60 patients (ASA Grade I/II) scheduled for various planned surgeries on hand, forearm and arm, under US-guided supraclavicular approach of brachial plexus block, was carried out.
|
Group |
Dose |
|
B |
Inj. Bupivacaine 0.5% 23ml + Inj. NS 0.9% 2ml |
|
D |
Inj. Bupivacaine 0.5% 23ml + Inj. Dexamethasone 2ml |
Patients with complete sensory and motor block were included in study.
• The demographic profile of the patients and duration of surgery was comparable among the groups. (p>0.05)
• Parameters were noted in the form of mean ± SD. A ‘p’ value of <0.05 was considered as statistically significant.
• The mean time of onset of sensory block in Group B was 5.10 ± 0.92 min. and Group D was 3.90 ± 0.84 min. (P<0.001)
• The mean time of onset of motor block in Group B was 6.50 ± 0.82 min. and Group D was 5.50 ± 1.04 min. (P<0.001)
• The mean time to achieve peak sensory block in Group B was 11.50 ± 0.78 min. and Group D was 9.40 ± 0.93 min. (P<0.001)
• The mean time of achieve peak motor block in Group B was 15.87 ± 1.17 min. and Group D was 12.30 ± 1.32 min. (P<0.001)
• The mean time of duration of motor block in Group B was 460 ± 22.89 min. and in Group D was 598.17 ± 28.05 min. (P<0.001)
• The mean time of duration of sensory block in Group B was 510±17.86 min. and in Group D was 807.5±24.45 min. (P<0.001)
• The mean time for 1st rescue analgesia in Group B was 580 ± 24.91 min and in Group D was 1010 ± 40.66 min. (P<0.001)
• Baseline hemodynamic variables like heart rate, blood pressure and SpO2 were stable and comparable in both the groups (p>0.05).
• No major complications and adverse events in perioperative period were noted in either group. Only one patient from Group B had shivering in intraoperative period.
• The addition of Dexamethasone to local anaesthetics (Bupivacaine) supraclavicular approach of brachial plexus block prolongs the duration of sensory, motor and time for requirement of 1st rescue analgesic.
To conclude with addition of Dexamethasone with inj. Bupivacaine 0.5% as an adjuvant in supraclavicular brachial plexus block hastens the onset and time to achieve peak of sensory and motor blockade, prolongs the duration of both blockades, delays the need of rescue analgesia compare to Inj. Bupivacaine 0.5% alone without notable any intraop and postop complications with stable hemodynamics [41,42].