



Case Report - (2016) Volume 1, Issue 1
A Catastrophe Caused by Central Venous Catheter Insertion: A Case Report
Received Date: Nov 01, 2016 / Accepted Date: Nov 13, 2016 / Published Date: Nov 17, 2016
Copyright: ©Almaghraby A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Central venous catheterization (CVC) is a routine technique done in critical care and emergency departments for monitoring patients and giving certain parenteral medications in special conditions. Most common complications associated with CVCs are infection, hematoma, hemothorax, pneumothorax and superior or inferior vena cava trauma while rare complications include cardiac arrhythmias, air embolism and loss of the guide wire [1]. We are reporting a case of unrecognized loss of CVC guide wire that caused a very rare unexplained cardiac complication.
Key Points
Central, Tricuspid, Valve, Complications
Introduction
Central venous catheterization (CVC) is a routine technique done in critical care and emergency departments for monitoring patients and giving certain parenteral medications in special conditions. Most common complications associated with CVCs are infection, hematoma, hemothorax, pneumothorax and superior or inferior vena cava trauma while rare complications include cardiac arrhythmias, air embolism and loss of the guide wire [1].
We are reporting a case of unrecognized loss of CVC guide wire that caused a very rare unexplained cardiac complication.
Case Report
A 50-year-old male patient with no previous medical history presented to our hospital complaining of high grade fever with gradual onset and stationary course with no response to antipyretics and antibiotics for 1 week.
Work-up for fever was unremarkable, mild renal impairment was accidentally diagnosed with Creatinine level of 2.8 mg/dl, fever subsided after giving intravenous antibiotics for 3 days then the patient developed hypotension, blood pressure was 70/40 mmHg, heart rate was 140 beats per minute, electrocardiogram showed sinus tachycardia, liver enzymes were elevated, serum bicarbonate level was very low so the intensive care specialist inserted a central venous catheter to guide his fluid status control, central venous pressure was very low so he received intravenous fluids together with the antibiotics.
Chest X-ray was done a day later after central venous catheter insertion and astonishingly we found the introducing guide wire left inside his heart starting from the right internal jugular vein towards the right atrium and ventricle making a loop inside the pulmonary artery then down through the inferior vena cava towards the hepatic vein. The lost wire was retrieved blindly without fluoroscopic guidance and follow-up X-ray showed no residual wire parts, then he was referred to us for echocardiography and we found severe tricuspid valve regurgitation with no signs of chronicity with perforation of the anterior leaflet, no visible vegetations or thrombi, right and left ventricular systolic and diastolic functions were completely normal and no pericardial effusion.
Two days later the patient was referred to us again for follow up as he was still hypotensive with elevated central venous pressure. The new echocardiography revealed severely reduced left ventricular systolic function with borderline dimensions and reduced right ventricular systolic function with normal dimensions.
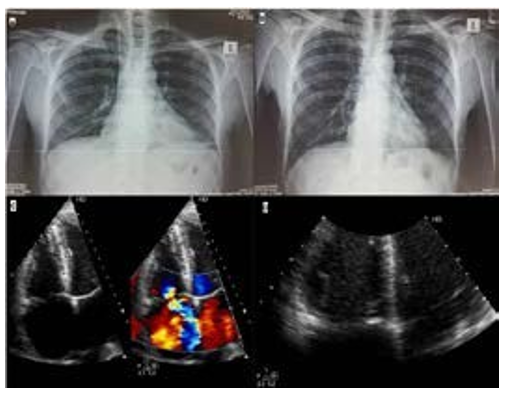
Figure 1: A: Chest X-ray showing the CVC insertion wire left inside the right side of the heart making a loop in the pulmonary artery then down to the hepatic veins. B: Chest X-ray after removal of the lost wire. C: 2D Echocardiography with color compares showing the severe tricuspid valve regurgitation. D: 2D Echocardiography for a zoom image on the tricuspid valve during diastole showing the perforated leaflet.
Discussion
To our knowledge, this is the first reported case of Tricuspid valve perforation and regurgitation after CVC insertion and lost guide wire. Also by reviewing the available literature, there is no known explanation for the development of heart failure in this reported case.
Conclusion
Although CVC insertion complications are very rare, we should take extreme care during insertion and maintenance, CVC insertion complications are preventable if we follow the precautions for safety during insertion such as:
• Good inspection of the guide wire before insertion for industrial defects.
• Fine manipulation of the guide wires, if resistance is met we should not apply more force and re-position the introducer.
• Always make sure that the outer part of the wire is under your vision.
• Always inspect the wire after removal to make sure that there are no missing parts inside the patient.
References
1.Akmal AH, Hasan M, Mariam A (2007) The Incidence of Complications of Central Venous Catheters at an Intensive Care Unit. Annals of Thoracic Medicine 2: 61-63.