




Case Report - (2024) Volume 3, Issue 3
A Case of Conjunctival Rhinosporidiosis Mimicking Squamous Papilloma in Ethiopian Child
2Aksum University College of Health Science Department of Ophthalmology, Aksum, Ethiopia
3Aksum University College of Health Science Department of Pediatrics and child health, Aksum, Ethiopia
Received Date: Sep 10, 2024 / Accepted Date: Oct 14, 2024 / Published Date: Oct 22, 2024
Copyright: ©2024 Birhanu Kassie Reta, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Reta, B. K., Weldegebriel, M. H., Hagos, H. H., Abebe, M. T. (2024). A Case of Conjunctival Rhinosporidiosis Mimicking Squamous Papilloma in Ethiopian Child. J Surg Care, 3(3), 01-03.
Abstract
Rhinosporidiosis is chronic granulomatous inflammation caused by a fish parasite called mesomycetozoa, which is usually acquired by traumatized mucosa primarily nasal mucosa. Ocular rhinosporidosis is uncommon even though reported cases are available. We present case of conjunctival rhinosporidosis in a 17-year-old male adolescent who presented with a complaint of conjunctival mass of 8 years duration. The histopathologic examination confirmed rhinosporidosis. This case report aims to highlight that conjunctival rhinosporidiosis can clinically mimic squamous papilloma and that cases of conjunctival rhinosporidiosis may present as mass lesions that persist for many years.
Keywords
Rhinosporidosis, Conjunctival, Squamous Papilloma, OcularAbbreviations
H and E-Hematoxylin and EosinIntroduction
Rhinosporidiosis is a chronic granulomatous inflammation caused by an aquatic protistan parasite called Rhinosporidium Seeberi [1-7]. Rhinosporidium seeberi is newly grouped as a fish parasite class called mesomycetozoa, which includes a heterogeneous group of microorganisms at the animal-fungal boundary[3, 5, 6]. Rhinosporidiosis is claimed to be acquired through traumatized mucous membranes, most commonly nasal mucosa, due to contact with water sources containing the parasite[1-3, 6-17]. Extranasal involvement is rare. Some of the extranasal sites affected by rhinosporidosis are ocular structures, lips, uvula, palate, trachea, pharynx, and bone [3, 6, 11]. The most commonly involved ocular structures are the conjunctiva, lacrimal sac, and sclera [2, 7-10]. The first case of ocular rhinosporidiosis, specifically conjunctival rhinosporidiosis, was reported in India in 1912 [5]. Nowadays several cases of ocular rhinosporidosis are reported in published case reports from Asia, Europe, and South American countries. Most cases of ocular rhinosporidosis are reported from Siri Lanka, Nepal, Bangladesh [3, 5, 6, 13]. In Africa, few cases of ocular rhinosporidiosis are reported in Kenya, Congo, Zambia, Tanzania, Ivory coast, and south Africa [3, 5]. In Ethiopia there is only one reported case of ocular rhinosporidosis to best of our knowledge [2].
Clinically patients with ocular rhinosporidosis present with slowly growing pinkish pedunculated or sessile polypoid mass, which is usually friable [3]. In addition to the mass lesion, they also complain of foreign body sensation, irritation, and watering of the eyes[2, 3, 5-7].
Diagnosis of rhinosporidosis is usually made through histopathologic examination, which classically demonstrates epithelial and subepithelial variably sized thick-walled sporangia containing numerous endospores eliciting inflammatory response consisting of mononuclear and polymorphonuclear infiltrates with occasional granuloma formation [2-6].
Case Presentation
History and Physical Examination
This is a 17-year-old adolescent male who presented to the ophthalmology clinic of Aksum University comprehensive specialized Hospital with a complaint of painless mass over his left eye of 8 years duration which was slowly growing. He had a history of frequently bathing and swimming in stagnant waters and lakes. Otherwise, the patient has no history of reduction in vision, redness of eye, bloody tears, trauma or surgery to his eye. No history of similar lesion in other parts of his body. On physical examination, visual acuity was 20/20 in both eyes which is normal. He had left lower palpebral conjunctiva soft to firm non tender fleshy pedunculated polypoid mass measuring 25mm*16mm. With the clinical diagnosis of conjunctival papilloma excisional biopsy was done and sent for histopathologic examination.
Histopathologic Finding
Skin-covered polypoid tissue without stalk measuring, 14mm*0.8 mm*0.6mm, was received. The cut surface was pinkish to purplish glistening with microcystic spaces. No solid focus was identified. The microscopic examination revealed non keratinizing squamous epithelium with interspersed goblet cells, lined tissue with underlying submucosal stroma displaying variable sized thick-walled sporangia filled with numerous sporangiospores with surrounding extensive mononuclear inflammatory infiltrate composed of lymphocytes, plasma cells and macrophages (Fig. 1 and 2). The sporangia are seen within the conjunctival mucosa, some of them bursting the spores. The submucosa also demonstrated numerous cysts devoid of spores.
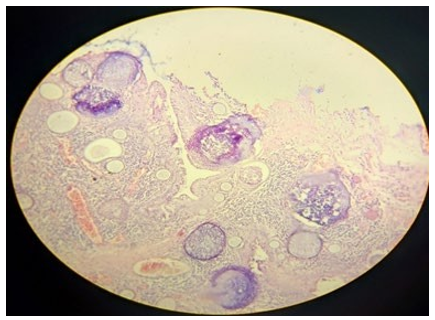
Figure 1: 4x Magnification Showing Conjunctival Epithelium Lined Tissue Displaying Epithelial and Submucosal Variable Sized Thick Sporangia Filled with Endospores and Empty Cysts Devoid of Endospores

Figure 2: 4x Magnification Displaying Variable Sized Sporangia Filled with Endospores with Surrounding Extensive Mixed Inflammatory Infiltrate
Discussion
Rhinosporidosis is a chronic granulomatous inflammatory condition caused by Rhinosporidium seeberi, which is acquired by bathing or contact with stagnant water, containing the parasite, with traumatized mucosa. The major risk factor for rhinosporidosis is bathing in rivers, lakes, or stagnant waters [2, 3]. Individuals within the second decade of life are usually affected by rhinosporidiosis, and approximately 7% of cases originate from conjunctival sources[2]. Our patient is from a rural part Tigray region, Ethiopia, where many rivers and lakes are found, and he claimed he had history of frequent bathing and swimming in rivers and stagnant water. In most of the reported cases of ocular rhinosporidosis, the duration of the conjunctival mass lesion ranges from 1 week to 16 months [1-14], which is relatively short compared to our case. In our instance, the mass lesion persisted for 8 years. The mass lesion in rhinosporidiosis is usually fleshy vascular polypoidal and mostly friable, which can be sessile or pedunculated.
The mass in our case was a pedunculated polypoid mass in the lower palpebral conjunctiva. Histological examination of the lesions classically shows variable sized thick sporangia containing endospores, eliciting mixed inflammatory responses [2, 7]. In our case, the H and E examination revealed conjunctival epithelium lined polypoid mass displaying numerous epithelial and submucosal thick sporangia containing endospores some of them ruptured, some submucosal cysts devoid of endospore and extensive inflammation consisting of neutrophils, mononuclear inflammatory cells of lymphocytes, plasma cells and histiocytes. (Fig 1 and 2). The ophthalmologist initially did not consider rhinosporidiosis as a diagnosis, as there were no much reported cases of conjunctival rhinosporidiosis in our country. Instead, due to the polypoid nature of the lesion and its prolonged duration, the clinical diagnosis was conjunctival papilloma.
Conclusion
For patients presenting with polypoid mass lesions in the conjunctiva or other ocular structures, rhinosporidiosis should be considered, particularly in those with a history of bathing or swimming in rivers or stagnant water. While most reported cases of rhinosporidiosis have a short duration of the mass lesion, they can also present after many years. Histopathologic confirmation is mandatory for diagnosis.
Follow-up
The patient was advised not to bath or swim in stagnant waters or lakes and to have subsequent follow-up to see if there is any recurrence.
Author Contribution
Birhanu Kassie Reta, Conceptualization; data curation; project administration; visualization; writing – original draft; writing – review and editing. Micheale Hailu Weldegebriel: Writing – original draft; writing review and editing. Hindeya Hailu Hagos: Data curation; investigation; writing – original draft. Mizan Tsegaye Abebe: Supervision; writing review and editing; visualization
Acknowledgment
We would like to express our gratitude to the patient and their family for permitting us to write this case report.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed consent
Written informed consent was obtained from the patient’s family for anonymized patient information to be published in this article.
Funding source
This study did not receive any grants or funding from either for- profit or non-profit organizations.
Data availability
The patient’s data and file are available.
Ethics statement
This is a case report and therefore did not require ethical approval from the ethics committee.
References
- Arias, A. F., Romero, S. D., & Garcés, C. G. (2021). Case report: rhinosporidiosis literature review. The American Journal of Tropical Medicine and Hygiene, 104(2), 708.
- Desta, T. W., & Kedir, A. (2022). Conjunctival rhinosporidiosis in an Ethiopian child: a case report. International Medical Case Reports Journal, 405-408.
- Ulzen-Appiah, K., Imbeah, E. G., Brookman, S. B., & Akakpo,P. K. A. (2022). A Rare Case Of Conjunctival Rhinosporidiosis Mimicking A Neoplasm In Ghana. Postgraduate MedicalJournal of Ghana, 11(2), 127-131.
- Doddawad, V. G., Singh, R., & Shivananda, S. (2022). A new technique to resolve Nasal Rhinosporidiosis: A case report with review of literature. International Journal of Surgery Case Reports, 92, 106807.
- Gichuhi, S., Onyuma, T., Macharia, E., Kabiru, J., Zindamoyen, A. M. B., Sagoo, M. S., & Burton, M. J. (2014). Ocular rhinosporidiosis mimicking conjunctival squamous papilloma in Kenya–a case report. BMC ophthalmology, 14, 1-4.
- Adhikari, A., Dutta, J., Das, S., Barua, N., Chakraborti, C., & Chakraborti, P. B. (2022). Ocular Rhinosporidiosis and Recurrence Postsurgery: A Case Series. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH, 16(1), NR01-NR03.
- Shah, S., Lavaju, P., Bharati, P., & Joshi, I. (2017). A case report of an unusual presentation of ocular rhinosporidiosis as a conjunctival cystic mass. Orbit, 36(1), 55-57.
- Sah, B. P., Chettri, S. T., Si, S., Kandel, D. R., & Ir, D. (2014).Lacrimal sac rhinosporidiosis: an unusual case report. Am JMed Case Rep, 2(4), 84-6.
- Shobita, Nair., Ravindran, A.V., Vinit, J. Shah., & Meenakshi. (2020). A Case Series of Conjunctival Rhinosporidiosis: Extremes of Presentation!! Acta Scientific Ophthalmology. 3(8): p. 57-60.
- Bhargava, M., Johri, A., Ghosh, A. D., Paul, R. S., Gupta, R., & Biswas, J. (2022). Conjunctival oculosporidiosis-associated ciliary staphyloma, managed with scleral patch graft using box sutures. Indian Journal of Ophthalmology-Case Reports, 2(1), 14-16.
- Chandran, A., Sakthivel, P., Kumar, R., & Rajeshwari, M. (2020). Pharyngeal rhinosporidiosis. BMJ Case Reports, 13(6).
- Bhagat, A., Singla, K., Singh, K., & Heer, P. (2020). Ocular rhinosporidiosis. QJM: An International Journal of Medicine, 113(7), 497-498.
- Reeta, Dhar., Gaikwad, P., & Sahu, S. (2019). Ocular Rhinosporidiosis - A Case Report. International Journal of Research and Review, September 2019. 6(9).
- Shilpy, N., & Mukherji, P. (2022). Ocular rhinosporidiosis-A case report. Indian Journal of Clinical and Experimental Ophthalmology. 8(2): p. 295-297.
- Vélez, A., Jiménez, G., Hidrón, A., Talero, S., & Agudelo,C. A. (2018). Rhinosporidiosis in Colombia: case series and literature review. Tropical Doctor, 48(4), 289-293.
- Tong, T. K., Ismail, I., Yunus Mohammad, N. M., Yusoff, S. M., & Sahri, A. M. (2023). Recurrent rhinosporidiosis: A case report from Malaysia and review of literature. Proceedings of Singapore Healthcare, 32, 20101058231160606.
- Penagos, S., Zapata, N., Castro, J. J., Hidron, A., & Agudelo,C. A. (2021). Rhinosporidiosis in the Americas: a systematic review of native cases. The American Journal of Tropical Medicine and Hygiene, 105(1), 171.