




Case Report - (2024) Volume 3, Issue 3
A Case of Breast Filariasis Diagnosed on Fine Needle Aspiration Cytology
2Arsi university College of health Science, Department of Pathology, Asella, Ethiopia
3Woldia University, Woldia, Ethiopia
4Addis Ababa University, College of Health Sciences, Addis Ababa University, Ethiopia
5Danat Hospital, Shire, Ethiopia
Received Date: Apr 11, 2024 / Accepted Date: Mar 12, 2024 / Published Date: Jun 12, 2024
Copyright: ©Â©2024 Birhanu Kassie Reta, et al. This is an open-ac-cess article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Reta, B. K., Tadesse, B. L., Kebede, E. G., Worku, A. B., Abera, M. T., et al. (2024). A Case of Breast Filariasis Diagnosed on Fine Needle Aspiration Cytology. J Surg Care 3(3), 01-03.
Abstract
The lymphatic system is the primary target of filariasis, which typically manifests as lymphedema due to lymphatic blockage. How- ever, filariasis may present in unusual locations, such as the skin and soft tissue, which is rarely documented. In this report, we describe a case of a 55-year-old woman who exhibited extra-lymphatic filarial infestation of the left breast. Fine needle aspiration cytology confirmed the diagnosis, revealing adult worms and embryonated eggs from a gravid female worm. This case is unique because of the infection's extremely unusual location.
Keywords
Breast Nodule, Lymphatic, Filariasis
Abbreviations
FNAC- Fine Needle Aspiration CytologyIntroduction
Lymphatic filariasis is a neglected tropical disease that causes severe disability and illness, primarily affecting impoverished communities with limited access to healthcare and sanitation. Filariasis is a chronic mosquito-borne parasitic infection with species of nematode parasites [1]. Filariasis is a widespread global health issue that results in socioeconomic instability in tropical regions across Asia, Africa, and South America [2-4]. In Ethiopia, lymphatic filariasis is particularly prevalent in the Gambella region, located in the western part of the country, with a reported prevalence rate of 3.7%. However, the prevalence in other regions of Ethiopia has not been well documented [5,6]. Filariasis primarily targets the lymphatic system, presenting with lymphedema and hydrocele [1]. Even if it is uncommon, filariasis has extra-lymphatic manifestations [7,8]. Among extra-lymphatic manifestations, breast involvement by filariasis is one of them with few documented case reports [9–11]. Fine needle aspiration cytology (FNAC) is a useful diagnostic method for detecting various stages of the infection. It usually identifies intact adult worms, microfilaria, embryonated eggs of gravid female worms, fragments of adult worms, and a mix of inflammatory cells, including eosinophils, lymphocytes, and occasionally granulomas [12,13].
Case History/Examination
A 55-year-old female patient from a rural area in northern Ethiopia presented with a complaint of a left breast lump and pain for 4 months. She also reported intermittent fever, generalized malaise, discharge from the swelling site, and a history of itching. Physical examination revealed a soft to firm, mobile subcutaneous mass in the left breast's upper outer quadrant. The overlying skin was erythematous, indurated, ulcerated, and oozing yellowish discharge (Figure 1). We noted multiple small, soft, mobile ipsilateral axillary lymph nodes, with the largest measuring 7 x 7 mm. The examination of the contralateral breast was unremarkable, with no history of nipple discharge or extremity edema. Her past medical and surgical history was unremarkable.Methods (Differential Diagnosis, Investigations, and Treatment)
A left breast ultrasound examination showed a 14 x 12 x 12 mm measuring well-defined irregular hypoechoic lesion with a surrounding hyperechoic rim in the upper outer quadrant within the peri-mammary subcutaneous layer, with a final impression of a subcutaneous abscess. The complete blood count showed a white blood cell count of 5.26 K/µL with elevated eosinophils (8% of total white blood cells and an absolute eosinophil count of 420 cells/µL). Eosinophilia was also confirmed by the peripheral blood film. Hemoglobin and platelet counts were within normal ranges. FNAC was conducted using a 21-gauge needle attached to a 5 ml disposable syringe, which yielded a yellowish pus. The aspirate was then smeared onto a slide, air-dried, and stained with Giemsa stain. Microscopic examination of the stained slides revealed intact adult worms, embryonated eggs of gravid female worms, fragments of the worms, and a mixture of inflammatory cells (Figures 2A-C). The primary impression of the caring physician was breast carcinoma, which is excluded after the cytology examination which did not reveal features of neoplastic condition.

Figure 1: Clinical Image of The Breast Lesion
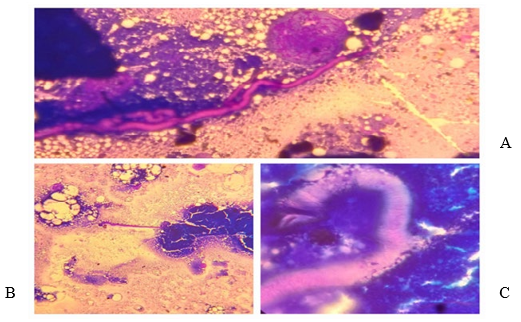
Figure 2: Cytologic Pictures
A and B: Adult Filarial Worm. C: Head of the Adult Filarial Worm.
Conclusions and Results (Outcome and Follow-Up)
We managed the patient with oral ivermectin and discharged her after a follow-up appointment. Although Diethylcarbamazine was our first choice, it was not available in our hospital. Upon follow¬up appointments the breast lump, skin induration, discharge as well as the generalized malaise and fever is resolved.Discussion
Filariasis is most commonly observed in Asia, especially in India, constituting about 20% of the total global burden [13]. Though filariasis is widespread globally, finding filarial worms in cytological smears is very rare [14]. The parasite primarily affects the lymphatic system, with clinical manifestations typically seen in the lower limbs, spermatic cord, and testis [1]. Filariasis has been reported in different extra-lymphatic organs, including the breast, thyroid, and epididymis, and infrequently, it can also be detected in soft tissue swellings, bone marrow, gynecologic smears, liver, and body cavity fluids [7,11,12,15]. Breast filariasis is rare, and when it does occur, the upper outer quadrant of the breast is the most frequent site, though it can affect any quadrant [9,11,16]. In this case, the filariasis was identified in the upper outer quadrant of the left breast.
Breast nodules due to filarial infestation are rare and can occasionally mimic malignant lesions [17,18]. In this case, the ulcerated nodule initially raised concerns about breast carcinoma. However, FNAC revealed fragments of adult worms, embryonated eggs of female worms, and a mix of inflammatory cells, which helped to settle the diagnosis of breast filariasis. In conclusion for patients presenting with breast nodules in filariasis-endemic areas, filarial nodules should be considered a differential diagnosis. Fine needle aspiration cytology is a crucial diagnostic tool for diagnosing filariasis and can help avoid unnecessary surgical procedures.
Acknowledgments
The authors have no acknowledgments to make.
Funding Information
The study did not receive any form of grant or funding from profit or non-profit agencies.
Conflict of Interest Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Consent
Written informed consent was obtained from the patient for anonymized patient information to be published in this article.
Ethics Statement
This is a case report and therefore did not require ethical approval from the ethics committee
References
- Newman, T. E., & Juergens A. L. (2024). Filariasis. StatPearls. Treasure Island FL ineligible companies. Disclosure: Andrew Juergens declares no relevant financial relationships with ineligible companies.: © 2024, StatPearls Publishing LLC.
- Eneanya, O. A., Garske, T., & Donnelly, C. A. (2019). The social, physical and economic impact of lymphedema and hydrocele: a matched cross-sectional study in rural Nigeria. BMC Infectious Diseases, 19, 1-16.
- Sawers, L., & Stillwaggon, E. (2020). Economic costs and benefits of community-based lymphedema-management programs for lymphatic filariasis in India. The American journal of tropical medicine and hygiene, 103(1), 295.
- Tyrell, E. (2013). Socioeconomic burden of lymphatic filariasis in G eorgetown, G uyana. Tropical Medicine & International Health, 18(2), 152-158.
- Shiferaw, W., Kebede, T., Graves, P. M., Golasa, L., Gebre, T., Mosher, A. W., ... & Hailu, A. (2012). Lymphatic filariasis in western Ethiopia with special emphasis on prevalence of Wuchereria bancrofti antigenaemia in and around onchocerciasis endemic areas. Transactions of the Royal Society of Tropical Medicine and Hygiene, 106(2), 117-127.
- Mengistu, B., Deribe, K., Kebede, F., Martindale, S., Hassan, M., Sime, H., ... & Kebede, B. (2017). The national programme to eliminate lymphatic filariasis from Ethiopia. Ethiopian medical journal, 55(Suppl 1), 45.
- Agarwal, K., Gaur, K., & Khasim, N. (2021). Filariasis presenting with bicytopenia, progressive splenomegaly and acute renal failure: An unusual case report. Tropical Doctor, 51(4), 588-590.
- Srinivasan, P., Ray, R., Jandhyala, S., & Agarwal, R. (2024). Extralymphatic Filariasis. Indian Dermatology Online Journal, 15(1), 92-94.
- Barwad, A., Singh, S. K., & Phulware, R. (2018). Breast filariasis. IDCases, 14, e00453.
- Trivedi, P. (2021). An Interesting Case of Bilateral Breast Filariasis. Sch J Med Case Rep, 2, 148-149.
- Kyaw, K. T., Myint, S. T., Thinn, K. K., & Lwin, T. (2021). Filariasis presenting as a breast lump. Breast Journal, 27(7).
- Gupta, D., Gupta, P., Jain, S., & Rahar, S. (2021). Cytological diagnosis of microfilariae in clinically unsuspected cases: a retrospective review of 12 cases. Cytopathology, 32(6), 807-812.
- Mondal, R. K., & Ghosh, S. (2019). Cytodiagnosis of Filariasis–A Retrospective Study of 8 Years.
- Goel, A., Agarwal, R., Mishra, J., Singh, N., & Deshmukh, G. (2017). Detection of Microfilaria on fine Needle Aspiration from Breast Lump: An Uncommon Finding. Annals of Pathology and Laboratory Medicine, 4(5), L19-20.
- Khandelwal, R., Agnihotri, N., & Pandey, S. (2018). Unanticipated cytodiagnosis of filariasis: A Study of 16 cases. Int J Med Res Rev, 6(03), 166-76.
- Sangwan, S., & Singh, S. P. (2015). Filariasis of the breast. medical journal armed forces india, 71, S240-S241.
- Gulati, M., Singla, V., Srinivasan, R., & Dahiya, D. (2024). A Word of Caution: a Case Report on Breast Filariasis Masquerading as Carcinoma. Indian Journal of Surgery, 86(1), 207-210.
- Kaur, R., Phillip, K. J., Masih, K., Kapoor, R., & Johnny,C. (2009). Filariasis of the breast mimicking inflammatorycarcinoma. Laboratory Medicine, 40(11), 683-685.