



Case Report - (2019) Volume 4, Issue 1
A Booby Trap Mitral Valve
Received Date: Mar 16, 2019 / Accepted Date: Mar 26, 2019 / Published Date: Mar 30, 2019
Copyright: ©Abdolazeem Elnour, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
The mitral valve and the mitral annulus can be considered a surgical trap by many uncommon surgical situations mainly in infective endocarditis, previous surgical intervention of the mitral valve, and/or calcification. All these scenarios can create a dangerous surgical Pathways and difficulties in replacing a prosthetic valve or annuloplasty ring. All mitral structural unit can be affected such as anterior or posterior mitral annulus, intervalvar fibrous body, sub-annular and Supra-annular tissues. This type of damage to the mitral valve can cause and lead to surgical challenges to any cardiac surgeons. We are presenting a case which reflects all these challenges clinically and surgically and our novel technique (modified anterior atrium sliding technique that we used to deal with it).
Introduction
Infective Endocarditis poses a huge challenge to most of the cardiac surgeons with other clinical situations such as calcification and previous surgical intervention. All these etiologies render the mitral valve as a very hostile region to deal with. Surgical debridement of calcified or infected mitral annulus or explantation of previous prosthesis can all make the mitral valve annulus friable, weak and sometime deficient, making it unstable for secure placement of a new mitral prosthesis [1]. When facing this type of pathological destruction of the mitral valve component will endanger patient’s life and leads to potentially disastrous complication such as ventricular rupture, uncontrollable bleeding and haemorrhage, atrioventricular disruption, and acute Myocardial Infarction due to damage to circumflex artery. Different surgical techniques where used to overcome this Fatal situation. Here we are concentrating mainly on our technique of repair used to the damaged, destroyed and eroded mitral annulus related to infective Endocarditis which rendered the valve replacement impossible.
Case Presentation
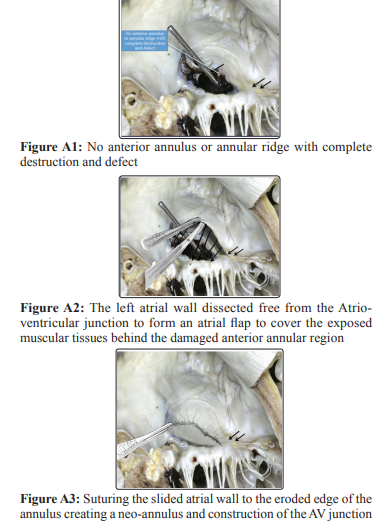
The patient was a 28 years old lady, with an unremarkable past medical history who was initially admitted for vaginal delivery which was uncomplicated. She was discharged but readmitted again after 5 days with a complaint of fever and cough. The first impression was that she is having chest infection. Blood cultures taken at that time showed growth of group A hemolytic streptococcus hence she received a course of intravenous antibiotics. She was discharged home after the I.V antibiotics, several days later readmitted again as her condition worsened with shortness of breath, orthopnoea and recurrence of fever. Patient received another course of injectable antibiotics. Further workup revealed that she is having a massive pericardial effusion with no features of tampnade in addition to bilateral pleural effusion. Valves were normal at that time. Patient was then referred to cardiothoracic surgery team where she underwent evacuation of the pericardial and pleural effusions via video assisted thoracoscopic (VAT) approach. She had smooth immediate post operative course. However, during routine follow up examination she was found to have a new murmur which was pansystolic. Bedside echocardiography showed severe mitral regurgitation with two jets; one was central and the other was through an anterior mitral leaflet defect (measuring 4.6 mm) near the annular base. There were no intra cardiac masses or thrombi. Another detailed echocardiography and transesophageal echo confirmed the previous findings. Consultation and workup by Rheumatology and chest medicine team ruled out the presence of any connective tissue disease or Tuberculosis. At this stage patient was haemodynamically stable and a febrile with the ongoing injectable antibiotics. Her inflammatory markers were unremarkable as well as her repeated 3 sets of blood culture result which showed no growth. However, in view of her previous fever with positive blood culture, and with this new mitral valve pathology, it was decided to treat the patient as a case of infective endocarditis hence she was started on combination antibiotic therapy for 4 weeks added to the previous two courses of antibiotic she already received. Thereafter, patient was referred again to cardiothoracic surgery team for surgical intervention as a case of valve endocarditis. During surgery it was found that there is severe destruction of the anterior leaflet with no annulus, annular ridge, ring or annular attachments. The leaflet has crescent-like feature, was hanging with two sites of attachments near the commissures only and the remaining of the leaflet was also deformed with complete defective anteroposterior continuity. Furthermore, the whole anterior mitral valve structure was eroded with severe destruction of the supra and infra annular row of tissues and structures (Figure A 1) [2]. The posterior leaflet was badly tethered with small perforation at its annular attachment. Therefore, there was no zone for prosthetic valve replacement or full annuloplasty ring. There was also a direct continuation of atrioventricular junction with erosion of AV sulcus.
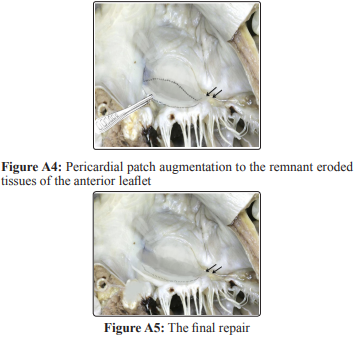
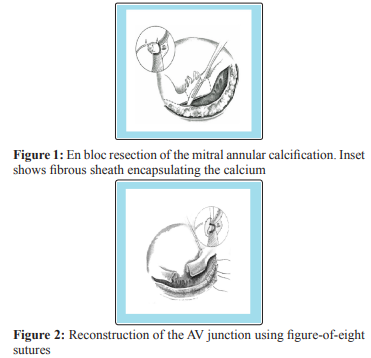
In addition to all these findings the endo and epicardial tissues were very poor and flimsy with lots of adhesions. Her ejection fraction was estimated to be around 35%. Since there was no possibility to replace the valve because of the previously mentioned anatomical defects, it was decided to repair as much as possible of that defective valve of both anterior and posterior leaflets. The left Atrium was dissected free from the Atrio-ventricular Junction to form an atrial flap to cover the exposed muscular tissues by suturing the slided atrial wall to the eroded edge of the of the annulus creating a neo-annulus, then the neo-annulus was sutured in continuation with the reconstructed anterior leaflet defect with a pericardial patch (Modified anterior atrium sliding technique) (Figures A2, 3, 4 and 5) [2]. The cleft between A1 and A2 was closed leaving a tiny cleft between A2 and A3 for venting, followed by a repair of the small perforation in the posterior leaflet and mobilization of posterior leaflet from its tethered position free. Finally inserting a partial posterior annuloplasty ring. The repair and the reconstruction were checked by Transesophageal echocardiography (TEE) and showed mild valve regurgitation which was considered satisfactory for this patient with all these severe anatomical abnormalities. Patient had smooth recovery after surgery and was hemodynamically stable but later on she developed a complete heart block for which a permanent pacemaker was inserted. Patient was then discharged in a good condition and followed up for more than one and a half year. Her final follow up echocardiography showed the same post-operative findings of mild mitral regurgitation.
Discussion
The surgical techniques or option in dealing with mitral annular destruction by infective endocarditis needs radical debridement which may leads to weakness and friability of the whole annulus and the surrounding tissues that makes the replacement of prosthesis very difficult and sometime impossible. In the literature, many descriptions of surgical techniques were published e.g. valve placement intra atrially or partially translocated into the left ventricle [3-6]. Alternatively it can be sutured to a new annulus structured using techniques mentioned by David and Feindel, Ergin et al., carpentier et al. [6-8]. Jault et al. found intra atrial placement of mitral prosthesis helpful when annular and sub-annular abscesses made traditional valve replacement difficult [9]. On the other hand, Lytle et al. and Udeken et al. stressed the importance of radical debridement of abscesses and reconstructed the annulus using autologous or bovine pericardium and they did not place the prosthesis extra anatomically [10, 11]. All these reports showed reasonable result in very high risk patients.
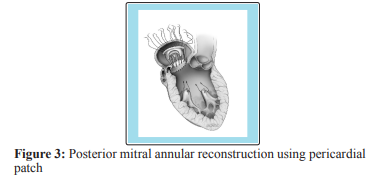
When reconstructing the mitral annulus most of the surgeons will do thorough debridement or decalcification. In case of calcified valve annular ring to create a supple mitral annulus for stable mitral valve replacement. Grossi et al. prescribed partial decalcification of the annulus in 64 patients [12]. They proposed debridement of calcium limited to the repair area and reconstruction of the annulus using non-pledgetted vertical figure of eight sutures. At the same time he demonstrated safety and durability of this technique with an operative mortality of 6.2% and 10 years freedom from reoperation of 88.1%. The complete debridement, decalcification and reconstruction of mitral annulus has been pioneered by Carpentier et al. by using techniques and procedures that have developed from the management of annular abscesses [6, 8]. Carpenter described excision of the calcium bar by sharp en- block dissection (figure 1), followed by mitral annular reconstruction using either figure of eight non-pledgetted suture (figure 2) or the sliding atrium technique [8].
David and colleagues reconstructed the posterior annulus using untreated autologous or glutaraldehyde bovine pericardial patch (figure 3) [13]. The patches provide fixation points for the prosthesis [6]. Using living vascularized issue leads to faster and stronger healing as carpentier’s group believe [8]. David’s group uses autologous untreated pericardium for repair of the posterior annulus and glutaraldehyde treated bovine pericardium or Dacron for reconstruction of the superior annulus and intravalvar body due to the strength of the materials [13, 14]. All these techniques in our opinion poses a life-threatening complications e.g. uncontrollable bleeding, injury to nearby structures e.g. circumflex artery, AV disruption and /or ventricular rupture if extreme cautions were not taken. We believe certain amount of surgical expertise is needed to overcome these complications [8]. In cases where endocarditis affecting the intervalvar fibrous body (IFB) some surgeons have preferred to suture the mitral and aortic valve sewing cuffs to each other. Suturing prosthesis together is not as secure as suturing them to a patch [6]. Endocarditis with abscesses in this anatomical Part may lead to ventriculo-aortic disruption and aorto-mitral discontinuity. David’s and Kraspolous group described a repair of this problem in 27 patients using custom structures valve Dacron conduit to rebuild and reconstruct the LVOT and the IFB (figure 4) [15]. The operative mortality was 11%. Follow up revealed no deaths, endocarditis, false aneurysms, or reoperation among Hospital survivors up to 7 years.
With regard to our case all the patho-anatomy which has been explained previously surgically we performed a major mitral valve reconstruction with reattachment of damaged and defective anterior leaflet to a neo-annulus reconstructed from anterior wall of the left Atrium ( modified sliding atrium technique) where the left Atrium is dissected free from the Atrio-ventricular Junction to form an atrial flap to cover the exposed muscular tissues, repair of the cleft between A1 and A2 and leaving a tiny cleft between A2 and A3 for venting, repair of the small perforation in the posterior leaflet and mobilization of posterior leaflet from its tethered position free and finally inserting partial posterior annuloplasty ring.
Conclusion
This type of destruction destructive pathology and anatomy of the mitral annulus is nothing other than a booby trap for any cardiac surgeon facing this kind of situations. We present these difficult surgical techniques in the literature and our favourite surgical option in such cases mainly in circumstances where any surgeon is not able to replace prosthetic valves because of destructive patho-anatomy. Our intention of sharing this case management is to be able to manipulate this very hostile event intra-operatively by careful and safe surgical technique and wise decision making.
References
- Lad VS, Newcomb AE, Davis PJ, Leng CY (2014) Surgical techniques for the Management of the ‘Hostile Mitral Annulus’. Heart, Lung & Circulation 23: 217-223.
- Cadaveric pictures for the purpose of illustrating the procedure.
- Mills NL, McIntosh CL, Mills LJ (1986) Techniques for management of the calcified mitral annulus. J Card Surg 1: 347-355.
- Nataf P, Pavie A, Jault F, Bors V, Cabrol C, et al. (1994) Intra atrial insertion of a mitral prosthesis in a destroyed or calcified mitral annulus. Ann Thorac Surg 58: 163-167.
- Nataf P, Jault F, Dorent R, Vaissier E, Bors V, et al. (1995) Extra annular procedures in the surgical management of prosthetic valve endocarditis. Eur Heart J 16: 99-102.
- Ergin MA, Raissi S, Follis F, Lansman SL, Griepp RB (1989) Annular destruction in acute bacterial endocarditis. Surgical techniques to meet the challenge. J Thorac Cardiovasc Surg 97: 755-763.
- David TE, Feindel CM (1987) Reconstruction of the mitral annulus. Circulation 76: III 102-107.
- Carpentier AF, Pellerin M, Fuzellier JF, Relland JY (1996) Extensive calcification of the mitral valve annulus: pathology and surgical management. J Thorac Cardiovasc Surg 111: 718-729.
- Jault F, Gandjbakhch I, Chastre JC, Levasseur JP, Bors V, et al. (1993) Prosthetic valve endocarditis with ring abscesses. Surgical management and long-term results. J Thorac Cardiovasc Surg 105: 1106-1113.
- Lytle BW, Priest BP, Taylor PC, Loop FD, Sapp SK, et al. (1996) Surgical treatment of prosthetic valve endocarditis. J Thorac Cardiovasc Surg 111: 198-210.
- d’Udekem Y, David TE, Feindel CM, Armstrong S, Sun Z (1996) Long-term results of operation for paravalvular abscess. Ann Thorac Surg 62: 48-53.
- Grossi EA, Galloway AC, Steinberg BM, LeBoutillier III M,Delianides J, et al. (1994) Severe calcification does not affect long-term outcome of mitral valve repair. Ann Thorac Surg 58: 685-687.
- David TE, Feindel CM, Armstrong S, Sun Z (1995) Reconstruction of the mitral anulus. A ten-year experience. J Thorac Cardiovasc Surg 110: 1323-1332.
- Feindel CM, Tufail Z, David TE, Ivanov J, Armstrong S (2003) Mitral valve surgery in patients with extensive calcification of the mitral annulus. J Thorac Cardiovasc Surg 126: 777-782.
- Krasopoulos G, David TE, Armstrong S (2008) Custom-tailored valved conduit for complex aortic root disease. J Thorac Cardiovasc Surg 135: 3-7.