
International Internal Medicine Journal(IIMJ)
ISSN: 2837-4835 | DOI: 10.33140/IIMJ
Impact Factor: 1.02



Case Report - (2025) Volume 3, Issue 2
Unconventional Manifestations of Pediatric Pneumonia: Clinical Insights into an Atypical Case
2American University of the Caribbean School of Medicine, Saint Kitts and Nevis- medical student, USA
3Mount Sinai Medical Center, United States, Emergency Medicine Physician D.O, USA
4St. George's University, Grenada- medical student, USA
5Ross University School of Medicine, Barbados- medical student, USA
6Alvis Pediatrics, United States- Pediatrician M.D, USA
Received Date: Feb 01, 2025 / Accepted Date: Feb 25, 2025 / Published Date: Mar 03, 2025
Copyright: ©©2025 Jovana Rutherford, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Rutherford, J., Moussa, M., Lamour, D., Santana, A., Javed, Z., Alvarez, I. (2025). Unconventional Manifestations of Pediatric Pneumonia: Clinical Insights into an Atypical Case. Int Internal Med J, 3(2), 01-04.
Abstract
Introduction: Atypical community-acquired pneumonia is a common yet potentially fatal infection in children, particularly when classical clinical signs and symptoms are absent.
Case Report: A 7-year-old Hispanic male with a history of developmental delay, umbilical hernia, and ADHD presented to the pediatrician’s office with a chief complaint of intermittent fevers and cough over the past 6 days. His parents reported that the fever recurred every other day, with temperatures ranging from 100-102°F, and claimed the onset of hives and swelling in the hands and feet on the 5th day. The patient had a negative screening for a rapid COVID, streptococcal, and influenza A/B test. He was sent to the hospital for a chest x-ray which revealed right upper lobe pneumonia. The patient received Azithromycin 200mg/5mL oral liquid 6.3mL on day 1 and 3.1mL for days 2-5 and Amoxicillin 400mg/5mL at 7mL q12h for 10 days, and loratadine 5mg/mL at 5 mg oral daily for 14 days.
Conclusion: One in five cases of pneumonia are atypical in the pediatric population with chances as high as 56% presenting asymptomatically which can make it challenging to diagnose.1 Classic presentation of atypical pneumonia present as the following: cough, fever, muscle ache. In this patient he presents with ambiguous symptoms. Patient followed-up two weeks later and reported abscess drainage on his head and he developed reactive adenitis. Outside of developing reactive adenitis due to an unrelated cause he recovered completely from the pneumonia. 10/25/24 - he developed reactive adenitis with 2 nodules noted on the superior region of head that was draining. He received clindamycin 75mg/5mL, 5ml TID for 10 days.
Keywords
Atypical Presentation, Pneumonia, Lobar Pneumonia
Introduction
Atypical pneumonia, also known as “walking pneumonia”, is a lung infection that can present with less severe symptoms than typical pneumonia. It can be caused by Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Influenza as well as opposed to Streptococcus pneumoniae. The symptoms of a typical pneumonia include elevated fever, productive cough with a green sputum, and lung sounds such as crackles, enhanced bronchophony, egophony, and tactile fremitus and a rapid onset of symptoms. In atypical pneumonia these symptoms have a subtler onset and the patient may have low-grade fevers and a non-productive cough persistent for several weeks. It can affect all age groups, however, is most common in school-aged children and young adults. Mycoplasma pneumoniae is the leading cause in children and has the highest incidence in schools and crowded environments.1 The use of standard antibiotics, which is used to treat typical pneumonia, will not be effective in treating the atypical bacterial organisms which can delay treatment. Recognizing atypical pneumonia can be challenging but is important because understanding the symptoms can lead to early detection and diagnosis.
Case Presentation
The patient was a 7-year-old Hispanic male with a significant medical history of developmental delay, umbilical hernia, and ADHD presented to the pediatrician’s office with a chief complaint of intermittent fevers and cough over the past 6 days. The patient initially returned home one evening from school and developed a fever in the evening of 100.3 degrees fahrenheit. The patient received a dose of motrin to manage his fever and the following day the fever disappeared. He continued to attend school regularly and was fine throughout the day. However, the next morning his fever reappeared and he had a persistent cough. The day afterwards his cough persisted, but his fever disappeared. On his 5th day of developing symptoms, the patient had a recurrent fever along with swelling of bilateral fingers. It was also noted by the mother that he had hives noted throughout his entire body. On the 6th day his fever subsided and the parents decided to bring their child to the pediatrician’s office out of concern for his intermittent fevers and unusual clinical presentation.
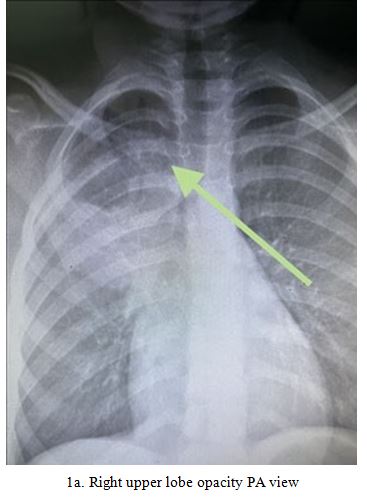
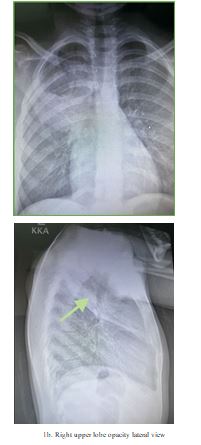
The patient appeared fatigued and his cough was reported to be resolving per parent. The patient appeared weak and his skin was notably dry and bilateral cheeks were red. On auscultation of his lungs, they were clear throughout, but was noted to have a dry cough frequently during the assessment. His cardiac exam was unremarkable. His peripheral pulses bilaterally were equal and palpable. Capillary refill was <3 seconds. The patient and family denied any diarrhea, altered mental status, weight loss, and hematuria. He was sent to have a posterior anterior chest x-ray with lateral views done the same day of the office visit. The results revealed a right upper lobe opacity consistent with right upper lobe pneumonia.
The patient received Azithromycin 200mg/5mL oral liquid 6.3mL on day 1 and 3.1mL for days 2-5 and Amoxicillin 400mg/5mL at 7mL q12h for 10 days, and loratadine 5mg/mL at 5 mg oral daily for 14 days. His symptoms resolved 2 weeks later during a follow- up visit in the pediatrician’s office. The patient appeared energized and was seen smiling at the office.
Discussion
Pediatric pneumonia is one of the leading causes of infection worldwide which can result in the demise of the pediatric patient.2 Pediatric pneumonia can be identified by the inflammation of alveolus which can be occluded by fluid or pus. There are many potential causes of infectious organisms which can contribute to the development of pneumonia depending on the age group of the patient. Classic presentations include fever, cough, fatigue, dyspnea, or even tachypnea.
Diagnosis of pediatric pneumonia can be made via clinical examination, history, and affirmed by a chest X-ray. It is important to rule out other contributing factors such as common viruses or streptococcal origins. Preventative measures can include up-to-date immunization, adequate nutrition, proper hand hygiene practices. If pneumonia is caught early enough and with adequate treatment most children will recover completely without any sequelae.
Conclusion
One in five cases of pneumonia are atypical in the pediatric population with chances as high as 56% presenting asymptomatically which can make it challenging to diagnose.1 Classic presentation of atypical pneumonia present as the following: cough, fever, muscle ache. In this patient he presents with ambiguous symptoms. Patient followed-up two weeks later and made a complete recovery without any sequelae. Providers should be aware of the various presentations of pneumonia which can complicate clinical diagnosis due to ambiguity of presentation. It is important to rule out other potential sources of infection prior to escalating approach.
Ethics Declaration
1. This case report did not require an IRB approval since this was not a study.
2. Consent was received to publish images and health information by patient’s parent presented on this manuscript.
Data Availability: Not applicable Competing Interest: Not applicable Funding Ddeclaration: Not applicable
Author Contribution
J.R. wrote abstract. M.M. wrote discussion. A.S. wrote introduction.
D.L. wrote case presentation. I.A. wrote conclusion. Z. J. wrote discussion and prepared figures 1a. and 1b. All authors reviewed manuscript.
Acknowledgments
I would like to extend my appreciation to Dr. Alvarez's team for their dedication and perseverance in providing outstanding care to their patients.
References
1. Edouard, S., Boughammoura, H., Colson, P., La Scola, B., Fournier, P. E., & Fenollar, F. (2024). Large-scale outbreak of Mycoplasma pneumoniae infection, Marseille, France, 2023– 2024. Emerging Infectious Diseases, 30(7), 1481.
2. unicef. (2021). Pneumonia in children Statistics-UNICEF DATA. UNICEF.