


Research Article - (2024) Volume 8, Issue 2
Ethical Pharmaceutical Practices and Beliefs in Lebanon: A National Cross-Sectional Study
2Community pharmacist, Member of the disciplinary board of the Lebanese Order of Pharmacists, Lebanon
Received Date: Nov 11, 2024 / Accepted Date: Dec 05, 2024 / Published Date: Dec 16, 2024
Copyright: ©2024 Aline Issa Barcha, et al. This is an open-ac-cess article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Barcha, A. I., Fadel, B. (2024). Ethical Pharmaceutical Practices and Beliefs in Lebanon: a National Cross-Sectional Study. J Addict Res, 8(2), 01-11.
Abstract
Background and Objectives: Pharmacy practice is in constant evolution. Ethical dilemmas are more often encountered and more complicated therefore the need to reform the code of pharmaceutical ethics in Lebanon is growing. Until today there has been no study investigating the ethical attitudes and beliefs among pharmacists and pharmacy students in Lebanon. The primary objective of this present study is to explore and understand pharmacists’ knowledge and attitudes towards ethics and good pharmacy prac- tice in daily experience in Lebanon and to determine the factors affecting these attitudes.
Methods: This was a cross-sectional study conducted among pharmacists and pharmacy students in Lebanon using a snowball sampling technique. An online questionnaire based on Google Forms was used to collect data. Descriptive and inferential analy- ses were conducted using SPSS statistics 26. Chi-square and Fisher exact tests were used. Tests were two-tailed and results with a p-value of ≤ 0.05 were considered statistically significant.
Results: Six hundred eighty-seven pharmacists and pharmacy students responded to the survey. Participants showed high im- plications in a patient-centered and collaborative approach (90%). The study shows financial pressure on pharmacists resulting in selling unneeded products (68%), selling products with the highest profit margin (57%) and below the official price (12%). Collaboration with other healthcare providers was a core standard in pharmacy practice (93%) and 47% assured the need for ongoing continuous education after licensure. The study shows the youngest age category having the highest agreement on continuous education being essential for maintaining licensure (65%, p=0.02). Pharmacists working outside Beirut and Mount Lebanon tend more to refuse overlooking expiry dates compared to other regions (77% vs 67%, p=0.017). Pharmacists working in the community pharmacy field tend to promote self-medication and sell unneeded products significantly more than those working in other pharmacy fields (p=0.001) and are significantly more implicated in personal development compared to other pharmacy fields (p=0.002).
Conclusion: The present study investigated the ethical practices of pharmacists in Lebanon shedding the light on challenges and dilemmas facing the pharmacist in daily practice. Further research on a large scale is needed helping to improve the code of ethics and guiding the Lebanese pharmacists in their daily practice.
Keywords
Ethical Practice, Pharmacist, Cross-Sectional Study, Questionnaire, Survey, Pharmacy Students, Lebanon
Introduction
Pharmacy ethics is a system of moral principles affecting pharmacists’ decisions in daily practice and ethical concern in pharmacy dates back to ancient civilizations as we see from the Hippocratic Oath [1,2]. Pharmaceutical care is defined as “the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve a patient’s quality of life” [3]. Since the pharmacy profession is increasingly evolving worldwide, the primary focus of pharmacists is shifting from products to patients and pharmacists are becoming also prescribers. Therefore, ethical dilemmas can occur between pharmacists and clients, pharmacists and physicians, and among pharmacists because the values, sense of justice, and fairness of each party may differ [4-7]. Moreover, not only a new set of technical skills is required, but also the negotiation of complex roles and relationships and changing patterns of accountability are essential to face contemporary challenges [8,9]. Research in ethical behavior and concerns mainly focuses on community pharmacists since they are more prone to ethical inquiries and when pharmacists allow business objectives to influence and control their conduct, the commitment to these concepts can be compromised therefore four main core values in community pharmacy practice were identified: commitment to the patient’s well-being, reliable and caring, pharmaceutical expertise and responsibility to society [1,10]. Pharmacy students are more and more integrated into ethical dilemmas and find in the textbook of pharmacy ethics a very helpful tool in guiding ethical decision- making [11]. Though there is no universal standard on pharmacists’ code of ethics, each country has a guideline on code of ethics and/ or code of conduct [12]. Studies on pharmaceutical practice and ethical behavior were mainly done in Anglo-Saxon countries (29/38) [13]. In the United Kingdom UK not only, pharmacists but also pharmacy students experience significant moral growth throughout the course of their studies [14]. The American Pharmacist’s Association AphA along with pharmaceutical associations in Australia, New Zealand as well as well in many countries like Iran and Canada published ethical guidelines and these guidelines were reviewed as a code of ethics for pharmacists to be respected and followed helping to ensure a good pharmacy practice [7,15].
The FIP statement of professional standards published in 2014 helped to guide pharmacists in their daily practice and society [16]. In Lebanon, guidelines for drug ethical standards in the marketing and promotion of pharmaceutical products are established by the Lebanese Order of Pharmacists (LOP) and the Ministry of Public Health in a code of drug ethical standards published in May 2016 and reviewed in the year 2018 (General clarification about the Lebanese code of ethics, moph) [17]. The code of ethics guiding pharmaceutical practice in Lebanon was first introduced in the year 2017 by the LOP and in the year 2019, the LOP was also able to generate and publish the first version of the Good Pharmacy Practice standards for community pharmacists in Lebanon [18]. However, due to the introduction of new challenges in today’s era, the need to reform this code of ethics is emerging as a necessity and the need to investigate the pharmacists’ perceptions of ethics and their behaviors in specific dilemmas is crucial to helping and guiding in this reform. Therefore, the main objective of this study was to explore and shed light on the ethical practices and beliefs of Lebanese pharmacists and pharmacy students in the modern era and in all sectors covering the relationship with the patient, the relation between colleagues, and other healthcare providers as well. As a secondary objective, the study aimed to assess factors influencing ethical practices and beliefs.
Material and Method
Study Design
This was an observational prospective cross-sectional study conducted among Lebanese pharmacists and pharmacy students between June 19 and August 26, 2024, aiming to explore the pharmacist’s ethical behavior towards his colleagues, his patients, and the society covering multiple challenges facing pharmacy practice in today’s era in Lebanon.
Inclusion and Exclusion Criteria
The study targeted the licensed Lebanese pharmacists currently practicing in Lebanon in all governorates and registered in the Lebanese order of pharmacists as well as the pharmacy students in their fifth year and above in Lebanese universities. A list of registered pharmacists in the Lebanese Order of Pharmacists (OPL) including full names of the pharmacists along with their phone numbers was used for this purpose. Pharmacists not practicing in Lebanon and not registered in the OPL as well as students below the fifth year were excluded from the study.
Sample Size
The minimal sample size was calculated using epi Info 7 Stat Calc functions for a population survey assuming that the prevalence of code of ethics acceptance in Lebanon is 50%. The minimal required sample size was calculated at a 95 % confidence interval using an absolute precision of 5 %. Thus, the calculated sample size for the current study to achieve a representative sample was 400 participants.
Sampling Method
Respondents completed an online survey using Google forms (https:// forms. gle/ fTTse Pe9sz 9cq82 p7). Survey was sent using phone numbers of pharmacists registered with the assistance of the OPL. As for the pharmacy students they were accessible through their corresponding faculties using their phone numbers and all faculties were approached: Saint Joseph University (USJ), Lebanese International University (LIU), Lebanese American University (LAU), Lebanese University, Beirut Arab University (BAU). To increase representativity of the sample we used the snowball sampling method assuring a fair distribution of participants according to region and field of work.
Questionnaire Development and Structure
The questionnaire was designed after a thorough literature review of relevant studies and after conducting group discussions with pharmacists aiming to explore the new challenges facing pharmacists in everyday practice and covering digital pharmacy practice, the relation between the pharmacist and his clients, between the pharmacist and his colleagues as well as other ethical dilemmas a pharmacist is facing during his practice. Questions were developed in three languages: Arabic, French and English aiming to maximize comprehension and participation of pharmacists. The questionnaire started with a small introduction: title, relation to the current disciplinary board of OPL, its purpose stating confidentiality and anonymity as well as the estimated time for completion of the questionnaire.
The introduction was followed by an informed consent statement and inclusion criteria then a set of questions (Lickert scale questions and closed questions) divided into 10 sections. The first section was dedicated to retrieving participants’ socio-demographic data, followed by nine sections assessing:
1. Professional integrity and patient care
2. Digital technology and pharmacy
3. Relationships with colleagues and the society
4. Conflict of interest
5. Professional competence
6. Hospital pharmacist’s ethical practice
7. Clinical pharmacist’s ethical practice
8. Case studies covering two ethical dilemmas
The questionnaire was revised and piloted by experts for its comprehensiveness, relevance, and ease of completion and a back translation was performed by a professional translator to ensure the right translation in the three languages: Arabic, French, and English.
Ethical Considerations
Being observational, voluntary, and respecting participants’ anonymity and confidentiality, the need for IRB ethical approval was waived. However, we ensured the approval of the ethical committee and the OPL board giving more credibility to the survey and aiming to access the largest number of pharmacists ensuring the diversity of the sample. Data was collected anonymously with no identifying or sensitive information.
Statistical Analysis
Descriptive and inferential analysis were conducted using Statistical package for the social sciences for Windows, Version 26.0 (IBM SPSS Statistics, Armonk, NY, USA). Categorical variables were summarized using frequency and percentages while using mean and standard deviations for the continuous variable age in years.
Bivariate analysis was performed using Chi square test or Fisher exact test for comparing distributions for the categorical variables. Tests were two-tailed and the level of significance for type one error was considered as 0.05.
Results
A brief description of the study and its importance and goals was displayed at the beginning of the survey. Respondents were informed that participation was optional, and data is anonymously analyzed. The data was downloaded anonymously from Google Forms in the form of an Excel sheet, and nothing could be used to uncover the identity of the participants. The questionnaire included 48 questions related to ethics in all pharmacy sectors other than socio-demographic data and two case studies.
Socio-Demographic Characteristics
Six hundred eighty-seven pharmacists responded to the online survey, among them eighteen were fifth year students or postgraduates. The mean age in years of our participants was 44 (12.11), ranging from 23 to 72 years, the highest category being less than 55 years (75%), and female (67.5%). Most participants (70%) were married, and most of them resided in Mount Lebanon (43%) and Beirut (19%) while 59% of the total participants were working in Beirut and Mount Lebanon. Most of respondents (97%) are registered pharmacists practicing in Lebanon and 71% are community pharmacists followed by hospital and clinical pharmacists and pharmaceutical companies (marketing, regulatory affairs, technical directors, quality control, consultancy). Pharmacy students accounted only for 3% of the total sample. Socio- demographic characteristics are summarized in Table 1.
|
Variable |
Categories |
Frequency (%) |
Mean (SD) |
|
Gender |
Male Femal |
223 (32.5%) 464 (67.5%) |
|
|
Age (years) |
|
na* |
44 (12.11) |
|
Age category |
[23-40] [40-55] ≥55 |
266 (38.8) 264 (38.5) 156 (22.7) |
na |
|
Marital status |
Married Single Other |
478 (70) 168 (24) 41(6) |
na |
|
Professional status |
Registered pharmacist Fifth year student or postgraduate |
669 (97.4) 18 (2.6) |
na |
|
Current main working region |
Bekaa Beyrouth Mount Lebanon North South Not concerned |
69 (10.0) 141 (20.5) 267 (38.9) 97 (14.1) 80 (11.6) 33 (4.8) |
na |
|
Current Working Region Category |
Beyrouth & Mount Lebanon All other regions |
408 (59.4) 279 (40.6) |
na |
|
Current working field category |
Community pharmacy Other Working fields |
485 (70.6) 202 (29.4) |
na |
|
na*: not applicable |
|||
Table 1: Demographic and Background Information of Respondents (N=687)
Professional Integrity and Patient Care
This section was dedicated to exploring the attitude of pharmacists towards the main principles of the pharmacists’ code of ethics exploring pharmacists’ ethical behavior and practice with the patient. Most pharmacists strongly agree with core ethical principles (90% and above), such as prioritizing patient care and refusing to participate in unethical practices (96% totally agree with ethical practices). However, attitudes towards promoting self- medication education showed more variability, with 52% fully agreeing, and 47% either partially agree or disagree.
Competing by selling medicine below its official price was accepted by 12% of participants. When pharmacists were asked about preserving honesty and integrity in daily practice with their patients, the majority stressed on the importance of ethical advertising (85%), and maintaining clean and healthy environment in the pharmacy (95%) whereas 77% of participants totally agreed on telling the truth and acting with conviction. Selling unneeded products to the patients was refused by 32% of participants while 88% would avoid discriminatory practice behaviors (Figure 1).
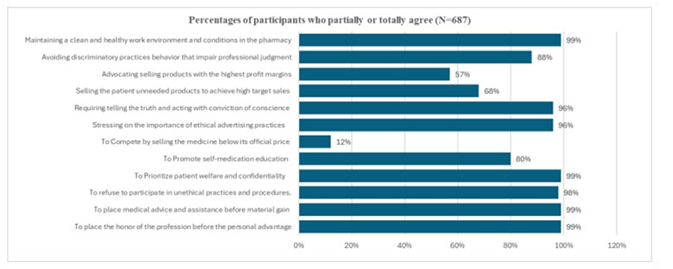
Figure 1: Professional Integrity and Patient Care: Percentages of Participants Who Partially or Totally Agree (N=687)
Relationships with Colleagues and the Society
The big part of participants (92%) focused on collaborative efforts rather than competing with their colleagues and were ready to share expertise and contribute to professional growth. Pharmacists showed respect for colleagues’ privacy (81%) and 75% considered “drug delivery” as a violation of the law of fair competition. Pharmacists showed ethical behavior when working with their colleagues by sharing expertise and competing while maintaining ethical behavior and participating in community health improvement (more than 90%). Pharmacists showed variability when asked about drug delivery showing 75% totally agreeing while 11% are against this service by pharmacist; majority of participants (92%) focused on personal and professional development only.
When asked about continuous education, 61% of participants find it optional but recommended, while 59% considered it essential for maintaining licensure and 62% believe that this requirement should not be limited to academic pharmacists only.
Digital Technology and Pharmacy
Tele pharmacy and digital health consultation have emerged as vital services therefore it necessitates adherence to professional standards and ethical practices. According to our participants, adherence to professional standards is mainly assured by protecting the patient data from misuse (61%), followed by assuring pharmacist’ availability and accessibility through teleconsultation (35%). (Figure 2).

The implication of participants in digital health showed 68% agreement that technology enhances patient care. Moreover, 72% agreed that technology revolutionized the way pharmacist interacts with patients, 76% agreed that the technology extends the reach of pharmacists beyond the traditional pharmacy setting and 81% believed that technology expands access to healthcare and medication counselling.
Conflict of Interest
Most participants believe that pharmacists should give priority to patient care over personal interests (96%) and should respect the law of practicing the profession of pharmacy (99%). Pharmacists always refer to a physician 45% of participants and 14% believe pharmacists should allow financial incentives to impact their professional advice.
Professional Competence
When choosing their priority of what should the code of ethics say about the necessity of maintaining and enhancing professional competence, 47% of participants supported the need for ongoing education after licensure through programs imposed by the order of pharmacists, 35% believed encouraging pharmacists to regularly assess and improve their professional skills, while 14% had a priority of collaborating with colleagues to address gaps in knowledge and skills and 3% believed that professional competence is less important than practical experience.
Environmental Sustainability in Pharmaceuticals
When asked about the implication of pharmacists in environmental sustainability, most participants believed actively promoting the use of biodegradable packing and medication take-back programs (92%), implementing drug recycling programs and developing eco-friendly drug formulations and packaging solutions (90%). While 88% do not encourage the prescription of higher doses to minimize frequency of purchases, and overlooking expiration dates to minimize wastage may be adopted by 23% of participants and 70% agree to dispose all pharmaceutical waste in common sites. Pharmacists encouraging patients to stockpile unused drugs for potential future use are approximately 30% of our participants and 78% may be opting for digital record in their daily practices.
Hospital Pharmacists
Most participants believe they should not falsify patient records to cover mistakes (94%), and they should discuss with other healthcare providers about patient’s medication (93%). While 26% of participants accept promoting brand-name drugs and conducting research for pharmaceutical companies, most participants (91%) do not accept to ignore potential drug interactions.
Clinical Pharmacists
In clinical pharmacy practice, priority in ethical responsibilities was given to reporting the treatments errors and collaborating to find a safe solution together with consulting with other healthcare providers about patient care as well as optimizing medication therapy for the best interest of the patient to promote their wellbeing (98% of participants). Promoting off-label use of medications and endorsing specific pharmaceutical brands was accepted by 14% of participants while only 42% consider following hospital policies without exception as priority.
Case Studies
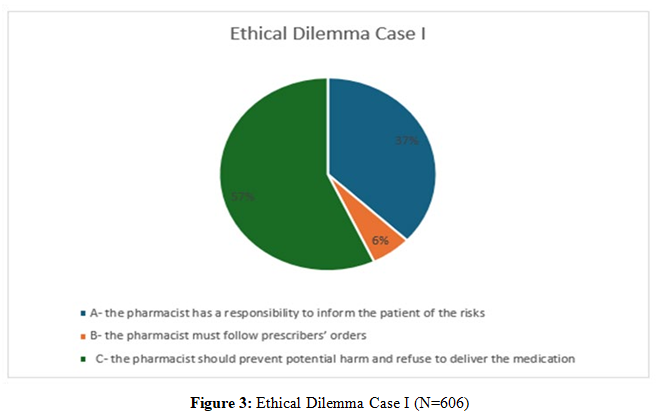
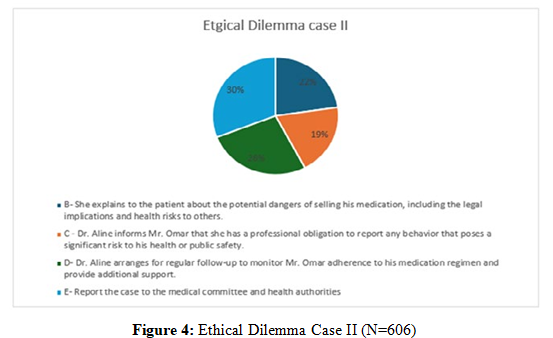
Half of our participants (50%) believed that the pharmacist should prevent potential harm and refuse to deliver medication whenever a prescribing error is discovered. When confronted with patients undergoing substance abuse 26% of participants believed that they should report the case to the medical committee and health authorities. (Figure 3,4).
Bivariate Analysis
A bivariate analysis was conducted to study the association between age category, working field (community pharmacist and other working fields), and working region (Beirut and Mount Lebanon and other areas) with ethical conduct and beliefs of pharmacists..
Age Categories
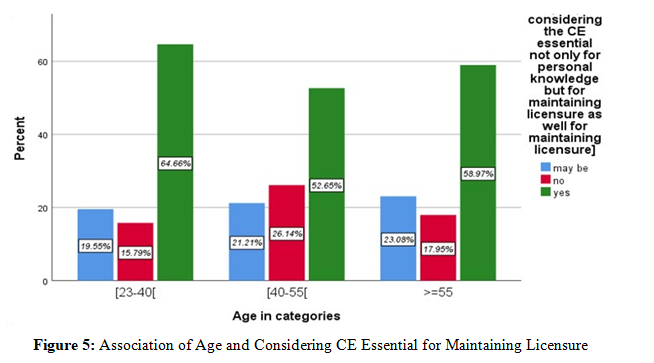
We studied the variability of answers across the three age categories: [23-40], [40-55], [55-73]. A highly significant difference (p≤0.001) was shown between the three age categories when asked about considering continuous education (CE) as optional but recommended: the highest level of disagreement in considering CE optional but recommended was in the youngest category showing 25% disagreement with this statement and this disagreement decreased with age, While 65% of the younger category of age had the highest total agreement that CE was essential for maintaining licensure showing concordance between these two answers (Figure 5).
When considering always referring to a physician’s opinion and if they follow hospital policies without exception, the difference between age categories was highly significant (p<0.001): answers showed 61% of the smallest age category not agreeing to always referring to a physician’s opinion. Significant differences were also found in considering the CE essential not only for personal knowledge but for maintaining licensure as well and the idea that technology extends the reach of pharmacists beyond the traditional community pharmacist setting and in encouraging patients to
stockpile unused drugs for potential future use. Among the pharmacists aged between 23 and 40 years 34% would encourage patients to stockpile drugs for potential future use and there was a statistically significant difference between age categories. Also, there was a significant difference among age categories when asked about following the hospital policies without exception, with the age category between 40 and 55 having the highest disagreement of 65%. Results of the bivariate analysis for the association between age and ethical behavior and practice are summarized in Table 2.
|
Variable |
Attitude and Beliefs |
Test |
p-value |
|
|
Age category |
Considering CE as optional but recommended |
Pearson Chi-Square |
0.001 |
|
|
[23-40[ [40-55[ ≥55 |
||||
|
Considering the CE essential not only for personal knowledge but for maintaining licensure as well |
Pearson Chi-Square |
0.02 |
||
|
Technology extends the reach of pharmacists beyond the |
Pearson Chi-Square |
0.01 |
||
|
|
traditional community pharmacist setting |
|
|
|
|
|
Pharmacist should always refer to the physician’s opinion |
Pearson Chi-Square |
0.001 |
|
|
|
Encouraging patients to stockpile unused drugs for potential |
Fischer’s Exact Test |
0.02 |
|
|
|
future use |
|
|
|
|
|
Following hospital policies without exception |
Pearson Chi-Square |
0.001 |
|
|
N.B Only tests with p-value ≤0.05 are exposed in this table |
|
|||
Table 2: Bivariate Analysis: Association of Age Category with Ethical Attitude and Beliefs of Study Participants (n=687)
Working Region Categories
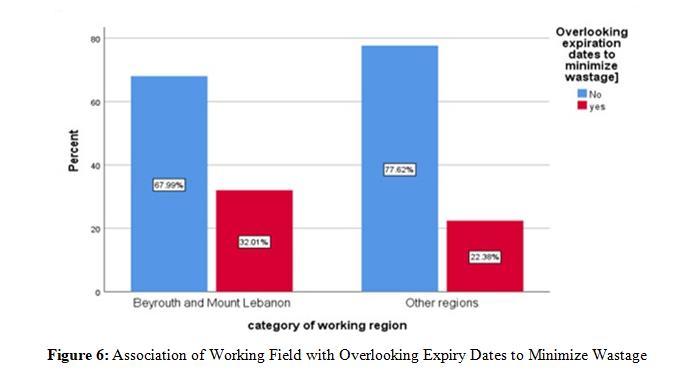
Significant divergence was shown between pharmacists working in Beirut and Mount Lebanon and the pharmacists working in the other regions when pharmacists were asked about continuous education: pharmacist working outside Beirut and Mount Lebanon were more in favor of considering it optional but recommended and the difference was significant (60% vs 57%, p=0.041) while 64% of those living in Beirut and Mount Lebanon did not agree of limiting this requirement to academic pharmacists vs 59% of those living in the other regions and this difference was significant (p=0.032). Overlooking expiry dates to minimize wastage was also significantly divergent between pharmacists working inside Beirut and Mount Lebanon and those working in the other regions: those working outside Beirut and Mount Lebanon refuse overlooking expiry dates in 77% of cases compared to 67% in the other group (p=0.017) (Figure 6).
Working Field
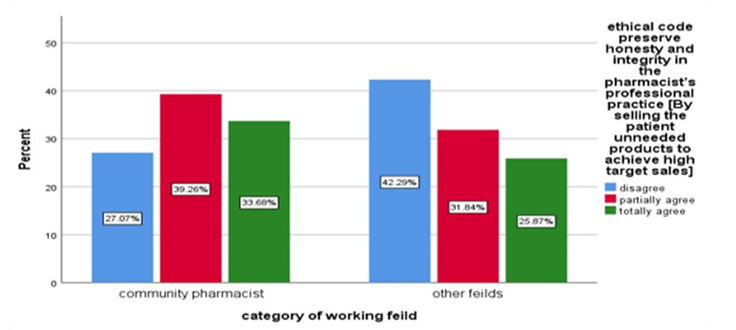
Some ethical considerations were significantly different between those who work in a community pharmacy and all other working fields: hospital and clinical pharmacists, industry related pharmacists, marketing and companies’ regulatory affairs, academicians as well as students. Results showed significant association between working field and promoting self-medication education: those working in community pharmacies are significantly more prone to promote self -medication (p=0.05) and are more in favor of considering continuous education as optional (63% vs 56%, p=0.05). Highly significant association was found between selling patients unneeded products to achieve higher target sales and the fact of being or not a community pharmacist (34% of community pharmacist accepts to sell unneeded products vs 26% of participants working in the other fields, p=0.002) (Figure 7). Moreover, community pharmacists showed more implication in focusing on personal development compared to other fields (39% vs 30%, p=0.002).
Results of the bivariate analysis for the association between working region as well as working field and ethical behavior and beliefs are summarized in table 3.
|
Variable |
Attitude and Beliefs |
Test used |
p-value |
|||||
|
Working region category |
Considering |
CE |
as |
optional |
but |
Pearson Chi-Square |
0.04 |
|
|
Beyrouth & Mount Lebanon |
recommended |
|
|
|
|
|
|
|
|
Other Regions |
||||||||
|
Limiting the requirement of ongoing |
Pearson Chi-Square |
0.03 |
||||||
|
|
education to academic pharmacists |
|
|
|||||
|
|
Overlooking expiration dates to minimize |
Fisher's Exact Test |
0.01 |
|||||
|
|
wastage |
|
|
|||||
|
Working Field category |
Selling the patient unneeded products to |
Fisher's Exact Test |
0.001 |
|||||
|
Community pharmacy |
achieve high target sales |
|
|
|||||
|
Other working fields |
||||||||
|
Focusing on personal and professional |
Focusing on personal and professional |
0.002 |
||||||
|
|
development only |
development only |
|
|||||
|
|
Following hospital policies without |
Pearson Chi-Square |
0.005 |
|||||
|
|
exception |
|
|
|||||
|
N.B Only tests with p-value ≤0.05 are exposed in this table |
|
|||||||
Table 3: Bivariate Analysis: Association of Working Region Categories and by Working Filled with Ethical Attitude and Beliefs of Study Participants (N=687)
Discussion
Based on a scoping review on pharmacy practice and clinical pharmacy research in the Middle East and to our knowledge, this is the first observational prospective cross-sectional study in the middle east region targeting all pharmaceutical sectors and aiming to explore ethical behavior and believes of pharmacists and pharmacy students in three directions: pharmacist and patient, pharmacist and his colleagues and pharmacist with medical and regulatory authorities providing a comprehensive analysis of pharmacists' knowledge and attitudes towards ethics and good pharmacy practice [19]. Pharmacists showed consistency and adherence to ethical behavior and patient care in terms of confidentiality and quality of service (more than 90%), the relation pharmacist-pharmacist as well (more than 90%) and sustainability by promoting eco-friendly solutions (90%) while partially showing interest in digitalization (76%) in their daily practice. Financial pressure may impact the ethical behavior of some pharmacists who are willing to compete by selling unneeded products to the patients (68%) allowing financial incentives to impact their professional advice (14%) and encouraging stockpiling and competing by selling medicine below official price (12%) while considering drug delivery not violating the law of fair competition among pharmacists (11%). Pharmacists showed high concern for patient confidentiality (61%) and were engaged in continuous education considering it essential for maintaining licensure (80%). When answering case studies, participants showed adherence to guidelines and regular authorities: the highest category (50%) believed in preventing potential harm and 26% would address regulatory authorities in case of suspicious clients. Moreover, the study shows the more pharmacists increase in age the more they give importance to continuous education. The category of pharmacists between 23 and 44 years was the most to encourage stockpiling medicine while those working in Beirut and Mount Lebanon were less prone to encourage overlooking medicine expiry dates compared to other regions.
The study shows community pharmacists are more prone to encourage self-medication highlighting the trend towards increased self-medication and self-care and selling unneeded products while they are more implicated in self-development compared to other working fields [20]. Our findings shed the light on the pivoting role of the Lebanese pharmacists in the health care system and this contrasts with the situation in Pakistan where the health care system has yet to recognize the pharmacist's role, and this lack of recognition is due to the limited interaction of pharmacists with the public [21]. Participants had different approaches when dealing with ethical dilemmas without dominant answer aligning with a study by Hibbert et al., 2011 in the United Kingdome showing that community pharmacists may respond to the same ethical dilemma in a different way [22]. This situation is acceptable since ethical dilemmas often have more than one right answer: there have been few international studies of the moral dilemmas experienced by community pharmacists, and existing studies vary widely in aim, method and presentation of results [10,22]. In Netherlands a study exploring ethical dilemmas confronting community pharmacists showed the relationship between the pharmacist, patient and other health professionals was complicated by other parties, such as legal representatives, health insurance companies, and regulators [10]. Most of the challenges of pharmacy practice are related to professionalism and professional commitment and ethical guidelines mainly target community pharmacists [23,24]. Research by Blenkinsopp et al., 1996 shows that community pharmacy is not profit motive predominated; a study on Swedish community pharmacists show that today's pharmacy is not focused on improving the use of medication, possibly resulting in the patient not gaining the most benefit from his or her treatment [20,25]. Also, an Australian survey on community pharmacist and interns showed interns reported more exposure to potential practice privacy breaches [26].
In pharmacy practice four ethical principles are measured and judged in interaction with one another: autonomy and beneficence of the patient, the principle of non-maleficence and finally the principle of justice [27]. Our study shows financial pressure affects ethical behavior and impacts pharmacists’ professionalism, and this is also shown in studies done in other countries: according to Salari et al., 2013 pharmacy students as well pharmacists in Iran are under the pressure of accepting a gift from pharmaceutical companies on their own. and confirmed the necessity of teaching the principles of professionalism in addition to providing an ethical guideline [7].
In Saudi Arabia, a study by Al Arifi et al. showed that only 43% of the community pharmacists would sell medication over the counter to a patient who does not really need it whereas in our study selling unneeded products to the patients was accepted by 68% of participants: both studies showed that pharmacists are struggling in their daily practice and the community pharmacists are under commercial pressure and more concerned about their own financial interests [2]. Our findings highlight the pharmacists’ professionalism in handling prescriptions by discussing with healthcare providers (93%) and referring to regulatory authorities (61%) and these findings align with the results of a cross-sectional study in Jordan on community pharmacists showing pharmacists tend to discuss and share decisions with their peers and healthcare professionals [1]. This is in contrast with what is found in a study by Rajiah et al., 2018 in India showing community pharmacists are in an extreme dilemma when handling a prescription from a physician though the medication prescribed is inadequate in therapeutic effect [12].
In terms of pharmacists’ discretion and respect for patient confidentiality our results aligned with those observed in Malta: 91% of consumers were satisfied with pharmacist discretion [28]. Patient confidentiality is a concern in rural pharmacists experiencing unique ethical dilemmas in relation to practice isolation, privacy, and confidentiality [9]. Moreover, most of the participants prioritized patient welfare (90%) and this finding aligned with the results of other research done by Benson et al when pharmacists ranked ‘patient welfare’ as the most important indicator of the quality of practice [8]. More recent research in Australia has also identified patient welfare as the core ethos underlying pharmacy practice [29]. There are often complex healthcare system pressures in the hospital setting that cause pharmacists to behave in ways that may conflict with professional values and behaviors [24]. A wide range of contemporary ethical issues unique to hospital pharmacy practice, mostly involving complex medication management safety, supply, and cost scenarios, were identified explaining the need for additional training, mentorship, and availability of hospital-specific targeted ethics resources therefore in Australia, hospital pharmacists rely on discussions with colleagues to brainstorm how to address ethical issues [24,30].
Strengths and Limitations
This present study has some limitations: the nature of the online survey as the Google Forms platform may induce selection bias but the fact that the survey was available in three languages made it accessible and comprehensive to all. Another limitation is the nature of the sampling method: snowball sampling allows the selection of some pharmacists over others. Moreover, the limited number of pharmacy students participating in the survey reduced its generalizability to Lebanese pharmacy students. Many strengths characterized this study mainly the large sample size, the relative representation of different geographical regions of Lebanon, and a strong representativity including all areas of practice and a broad spectrum of pharmacist specialties and age categories. The approval of the Lebanese order of pharmacists providing a list of registered pharmacists assured a sample frame and credibility of the results. More important was the comprehensiveness of the questionnaire, which was provided in three languages, assuring the questionnaire was understandable to all participants. These components allow the generalizability of the results to all Lebanese pharmacists making it a nationwide study.
Conclusion
This cross-sectional study revealed that Lebanese pharmacists have a strong commitment to ethical standards particularly in promoting patient well-being with collaboration and transparency seen as crucial elements of their role. Divergence is revealed in areas concerning profit-driven practices, promoting self-medication, and certain advertising standards shedding light on real-world pressures such as financial incentives and market competition that may challenge these ideals in practice. Continuous education on ethics, technology integration, and sustainability can help further strengthen ethical practices in pharmacy. Additionally, clearer guidelines on handling ethical dilemmas would help standardize responses across the profession. Further research on a large scale is needed in this area of practice to improve the code of ethics and to guide Lebanese pharmacists in their daily practice.
Acknowledgements
The author would like to acknowledge the assistance of Dr Joe Salloum (actual president of the Lebanese order of Pharmacists) as well as members of the disciplinary board: Dr Ziad ElHajj Chhade and Dr Vera Haidar. As well as all the Lebanese pharmacists for their support in achieving this survey. Special thanks to Dr Aida Farha, a referenced pharmacist and librarian.
References
1. Al-Qudah, R. A., Tuza, O., Tawfiek, H., Chaar, B., & Basheti, I. A. (2019). Community pharmacy ethical practice in Jordan: assessing attitude, needs and barriers. Pharmacy Practice (Granada), 17(1).
2. Al-Arifi, M. N. (2014). Community pharmacist perception and attitude toward ethical issues at community pharmacy setting in central Saudi Arabia. Saudi Pharmaceutical Journal, 22(4), 315-325.
3. Buerki, R. A. (2013). Pharmacy ethics: a foundation for professional practice.
4. Resnik, D. B., Ranelli, P. L., & Resnik, S. P. (2000). The conflict between ethics and business in community pharmacy: what about patient counseling? Journal of Business Ethics, 28, 179-186.
5. Kruijtbosch, M., Göttgens-Jansen, W., Floor-Schreudering, A., van Leeuwen, E., & Bouvy, M. L. (2018). Moral dilemmas of community pharmacists: a narrative study. International journal of clinical pharmacy, 40, 74-83.
6. Lowenthal, W. (1988). Ethical dilemmas in pharmacy. Journal of medical ethics, 14(1), 31-34.
7. Salari, P., Namazi, H., Abdollahi, M., Khansari, F., Nikfar, S., Larijani, B., & Araminia, B. (2013). Code of ethics for the national pharmaceutical system: Codifying and compilation. Journal of research in medical sciences: the oficial journal of Isfahan University of Medical Sciences, 18(5), 442.
8. Benson, A., Cribb, A., & Barber, N. (2009). Understanding pharmacists' values: A qualitative study of ideals and dilemmas in UK pharmacy practice. Social Science & Medicine, 68(12), 2223-2230.
9. Sim, T. F., Sunderland, B., & Hattingh, H. L. (2019). Exploring influences on pharmacists’ and students’ ethical reasoning in a changing practice landscape in Australia. International Journal of Clinical Pharmacy, 41, 280-288.
10. Kruijtbosch, M., Göttgens-Jansen, W., Floor-Schreudering, A., van Leeuwen, E., & Bouvy, M. L. (2019). Moral dilemmas reflect professional core values of pharmacists in community pharmacy. International Journal of Pharmacy Practice, 27(2), 140-148.
11. Buerki, R. A., & Vottero, L. D. (2002). Ethical responsibility in pharmacy practice. Amer. Inst. History of Pharmacy.
12. Rajiah, K., & Venkataraman, R. (2018). Community pharmacists’ perceptions on ethical dilemmas, pharmacy values and decision-making. Indian Journal of Pharmacy Practice, 11(4).
13. de Cursay, CL, Akliouat, N., Karamé, C., Gagnon-Lépine, SJ, Porteils, C., Brière, AL, & Bussières, JF (2021, July). Evaluating the ethics of pharmaceutical practices: a literature review. In Annales Pharmaceutiques Françaises (Vol. 79, No. 4, pp. 446–456). Elsevier Masson.
14. Gallagher, C. T. (2011). Assessment of levels of moral reasoning in pharmacy students at different stages of the undergraduate curriculum. International Journal of Pharmacy Practice, 19(5), 374-380.
15. Guérin, A., & Bussières, JF (2017, January). Pilot study of the level of agreement with statements on pharmaceutical ethics of pharmacy students and hospital pharmacists in Quebec. In Annales Pharmaceutiques Françaises (Vol. 75, No. 1, pp. 67-
76). Elsevier Masson.
16. FIP STATEMENT OF POLICY, 2014.
17. General clarification about the Lebanese code of ethics. Pdf
18. Hallit, S., Sacre, H., Sarkis, H., Dalloul, N., Abou Jaoude, C., Nahhas, Z., ... & Salameh, P. (2019). Good pharmacy practice standardized for community pharmacists: the lebanese order of pharmacist’s initiative. Journal of Research in Pharmacy Practice, 8(1), 29-32.
19. Obaid, D., El-Dahiyat, F., & Babar, Z. U. D. (2022). Pharmacy practice and clinical pharmacy research in the Middle East: a scoping review of studies from Bahrain, Iraq, Jordan, Kuwait, Lebanon, Oman, Palestine, Qatar, Saudi Arabia, Syria, United Arab Emirates, and Yemen. Journal of Pharmaceutical Policy and Practice, 15(1), 40.
20. Blenkinsopp, A., & Bradley, C. (1996). Over the Counter Drugs: Patients, society, and the increase in self-medication. Bmj, 312(7031), 629-632.
21. Azhar, S., Hassali, M. A., Ibrahim, M. I. M., Ahmad, M., Masood, I., & Shafie, A. A. (2009). The role of pharmacists in developing countries: the current scenario in Pakistan. Human Resources for Health, 7, 1-6.
22. Hibbert, D., Rees, J. A., & Smith, I. (2000). Ethical awareness of community pharmacists. International Journal of Pharmacy Practice, 8(2), 82-87.
23. Esmalipour, R., Larijani, B., Mehrdad, N., Ebadi, A., & Salari, P. (2021). The ethical challenges in pharmacy practice in community Pharmacies: A qualitative study. Saudi Pharmaceutical Journal, 29(12), 1441-1448.
24. McCleery, N., Caze, A. L., Winckel, K., & Hattingh, H. L. (2024). Evaluation of an interactive education workshop on hospital pharmacists’ ethical reasoning: an observational study. BMC medical ethics, 25(1), 81.
25. Olsson, E., Ingman, P., Ahmed, B., & Sporrong, S. K. (2014). Pharmacist–patient communication in Swedish community pharmacies. Research in Social and Administrative Pharmacy, 10(1), 149-155.
26. Hattingh, H. L., King, M. A., Hope, D. L., & George, E. (2019). Pharmacy ethical reasoning: a comparison of Australian pharmacists and interns. International Journal of Clinical Pharmacy, 41(4), 1085-1098.
27. Iranmanesh, M., Yazdi-Feyzabadi, V., & Mehrolhassani, M. H. (2020). The challenges of ethical behaviors for drug supply in pharmacies in Iran by a principle-based approach. BMC Medical Ethics, 21, 1-15.
28. Wirth, F., Tabone, F., Azzopardi, L. M., Gauci, M., Zarb- Adami, M., & Serracino-Inglott, A. (2010). Consumer perception of the community pharmacist and community pharmacy services in Malta. Journal of Pharmaceutical Health Services Research, 1(4), 189-194.
29. Chaar, B., Brien, J. A., & Krass, I. (2005). Professional ethics in pharmacy: the Australian experience. International Journal of Pharmacy Practice, 13(3), 195-204.
30. So, B., Tuche, M., King, M. A., Hope, D. L., La Caze, A., & Hattingh, H. L. (2021). Hospital pharmacists’ ethical exposure and decision-making. Research in Social and Administrative Pharmacy, 17(2), 372-380.